

Association of Intensive Care Unit Patient Load and Demand With Mortality Rates in US Department of Veterans Affairs Hospitals During the COVID-19 Pandemic
- PMID: 33464319
- PMCID: PMC7816100
- DOI: 10.1001/jamanetworkopen.2020.34266
Association of Intensive Care Unit Patient Load and Demand With Mortality Rates in US Department of Veterans Affairs Hospitals During the COVID-19 Pandemic
Abstract
Importance: Although strain on hospital capacity has been associated with increased mortality in nonpandemic settings, studies are needed to examine the association between coronavirus disease 2019 (COVID-19) critical care capacity and mortality.
Objective: To examine whether COVID-19 mortality was associated with COVID-19 intensive care unit (ICU) strain.
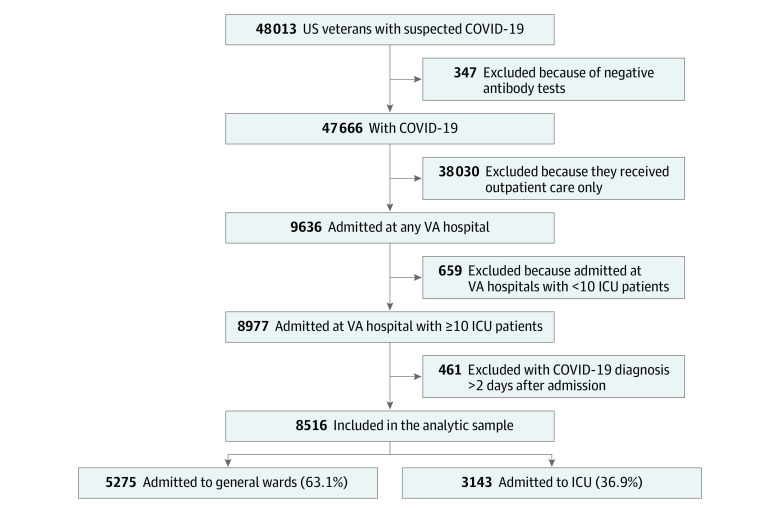
Design, setting, and participants: This cohort study was conducted among veterans with COVID-19, as confirmed by polymerase chain reaction or antigen testing in the laboratory from March through August 2020, cared for at any Department of Veterans Affairs (VA) hospital with 10 or more patients with COVID-19 in the ICU. The follow-up period was through November 2020. Data were analyzed from March to November 2020.
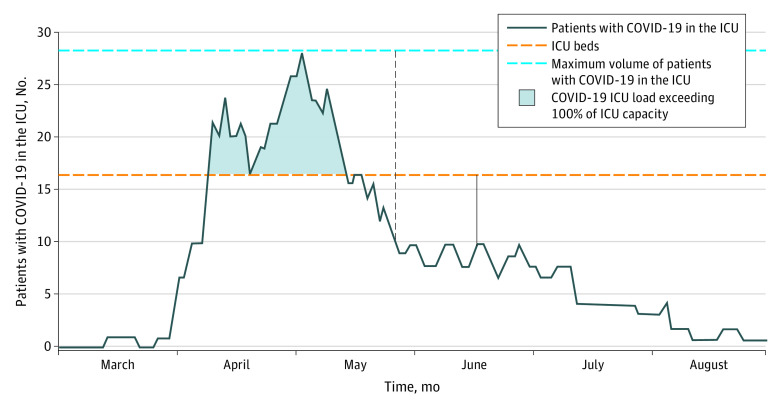
Exposures: Receiving treatment for COVID-19 in the ICU during a period of increased COVID-19 ICU load, with load defined as mean number of patients with COVID-19 in the ICU during the patient's hospital stay divided by the number of ICU beds at that facility, or increased COVID-19 ICU demand, with demand defined as mean number of patients with COVID-19 in the ICU during the patient's stay divided by the maximum number of patients with COVID-19 in the ICU.
Main outcomes and measures: All-cause mortality was recorded through 30 days after discharge from the hospital.
Results: Among 8516 patients with COVID-19 admitted to 88 VA hospitals, 8014 (94.1%) were men and mean (SD) age was 67.9 (14.2) years. Mortality varied over time, with 218 of 954 patients (22.9%) dying in March, 399 of 1594 patients (25.0%) dying in April, 143 of 920 patients (15.5%) dying in May, 179 of 1314 patients (13.6%) dying in June, 297 of 2373 patients (12.5%) dying in July, and 174 of 1361 (12.8%) patients dying in August (P < .001). Patients with COVID-19 who were treated in the ICU during periods of increased COVID-19 ICU demand had increased risk of mortality compared with patients treated during periods of low COVID-19 ICU demand (ie, demand of ≤25%); the adjusted hazard ratio for all-cause mortality was 0.99 (95% CI, 0.81-1.22; P = .93) for patients treated when COVID-19 ICU demand was more than 25% to 50%, 1.19 (95% CI, 0.95-1.48; P = .13) when COVID-19 ICU demand was more than 50% to 75%, and 1.94 (95% CI, 1.46-2.59; P < .001) when COVID-19 ICU demand was more than 75% to 100%. No association between COVID-19 ICU demand and mortality was observed for patients with COVID-19 not in the ICU. The association between COVID-19 ICU load and mortality was not consistent over time (ie, early vs late in the pandemic).
Conclusions and relevance: This cohort study found that although facilities augmented ICU capacity during the pandemic, strains on critical care capacity were associated with increased COVID-19 ICU mortality. Tracking COVID-19 ICU demand may be useful to hospital administrators and health officials as they coordinate COVID-19 admissions across hospitals to optimize outcomes for patients with this illness.
Conflict of interest statement
Figures
Comment in
-
Intensive Care Unit Strain and Mortality Risk Among Critically Ill Patients With COVID-19-There Is No "Me" in COVID.JAMA Netw Open. 2021 Jan 4;4(1):e2035041. doi: 10.1001/jamanetworkopen.2020.35041. JAMA Netw Open. 2021. PMID: 33464314 No abstract available.
References
-
- VA Health Services Research and Development VA Informatics and Computing Infrastructure (VINCI). Accessed December 10, 2020. https://www.hsrd.research.va.gov/for_researchers/vinci/default.cfmhttps://vaww.vinci.med.va.gov/VinciCentral/Home/About
-
- Borzecki AM, Wong AT, Hickey EC, Ash AS, Berlowitz DR. Can we use automated data to assess quality of hypertension care? Am J Manag Care. 2004;10(7 Pt 2):473-479. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
