

Gender differences in patient journey to diagnosis and disease outcomes: results from the European Map of Axial Spondyloarthritis (EMAS)
- PMID: 33464431
- PMCID: PMC8189938
- DOI: 10.1007/s10067-020-05558-7
Gender differences in patient journey to diagnosis and disease outcomes: results from the European Map of Axial Spondyloarthritis (EMAS)
Abstract
Introduction/objectives: To evaluate the journey to diagnosis, disease characteristics and burden of disease in male and female patients with axial spondyloarthritis (axSpA) across Europe.
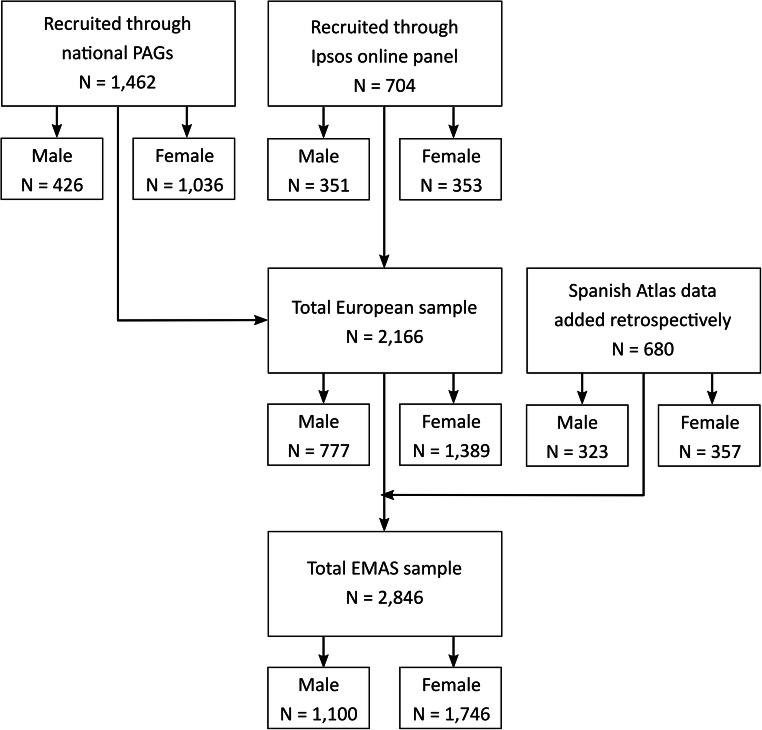
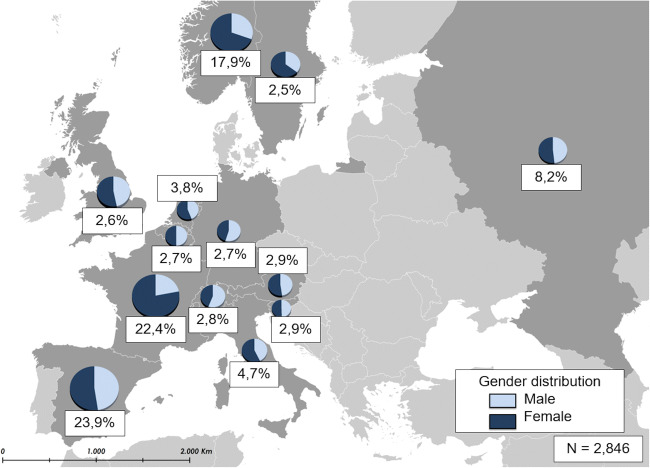
Method: Data from 2846 unselected patients participating in the European Map of Axial Spondyloarthritis (EMAS) study through an online survey (2017-2018) across 13 countries were analysed. Sociodemographic characteristics, lifestyle, diagnosis, disease characteristics and patient-reported outcomes (PROs) [disease activity -BASDAI (0-10), spinal stiffness (3-12), functional limitations (0-54) and psychological distress (GHQ-12)] were compared between males and females using chi-square (for categorical variables) and student t (for continuous variables) tests.
Results: In total, 1100 (38.7%) males and 1746 (61.3%) females participated in the EMAS. Compared with males, females reported considerable longer diagnostic delay (6.1 ± 7.4 vs 8.2 ± 8.9 years; p < 0.001), higher number of visits to physiotherapists (34.5% vs 49.5%; p < 0.001) and to osteopaths (13.3% vs 24.4%; p < 0.001) before being diagnosed and lower frequency of HLA-B27 carriership (80.2% vs 66.7%; p < 0.001). In addition, females reported higher degree of disease activity in all BASDAI aspects and greater psychological distress through GHQ-12 (4.4 ± 4.2 vs 5.3 ± 4.1; p < 0.001), as well as a greater use of alternative therapies.
Conclusion: The patient journey to diagnosis of axSpA is much longer and arduous in females, which may be related to physician bias and lower frequency of HLA-B27 carriership. Regarding PROs, females experience higher disease activity and poorer psychological health compared with males. These results reflect specific unmet needs in females with axSpA needing particular attention. Key Points • Healthcare professionals' perception of axSpA as a predominantly male disease may introduce some bias during the diagnosis and management of the disease. However, evidence about male-female differences in axSpA is scarce. • EMAS results highlight how female axSpA patients report longer diagnostic delay and higher burden of the disease in a large sample of 2846 participants of 13 European countries. • Results reflect unmet needs of European female patients. Healthcare professionals should pay close attention in order to accurately diagnose and efficiently manage axSpA cases while further research should be developed on the cause of reported gender differences.
Keywords: Axial spondyloarthritis; Europe; Gender; Patient journey; Patient-reported outcomes.
Conflict of interest statement
All the authors have received honoraria for participating in EMAS from Novartis Pharma AG.
Dr. Denis Poddubnyy has received unrelated research grants from Abbvie, Lilly, MSD, Novartis, and Pfizer, and unrelated honoraria from Abbvie, BMS, Celgene, Lilly, MSD, Novartis, Pfizer, Roche, and UCB.
Dr. Laure Gossec has received unrelated research grants from BMS, Lilly, and Pfizer and unrelated honoraria from Abbvie, BMS, Celgene, Janssen, Lilly, Novartis, MSD, Pfizer, and UCB.
Dr. Christine Bundy has received unrelated honoraria from Abbvie, Celgene, Janssen, Lilly, Novartis, and Pfizer.
Mrs. Souzi Makri has received unrelated honoraria or research grants from Bayer, GSK, Novartis and Pfizer.
Dr. Carlos Delgado Domínguez has received unrelated honoraria from Novartis.
Dr. Victoria Navarro-Compán has received unrelated honoraria or research grants from Abbvie, BMS, Lilly, MSD, Novartis, Pfizer, Roche, and UCB.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
