

Cervical Proprioception Impairment in Neck Pain-Pathophysiology, Clinical Evaluation, and Management: A Narrative Review
- PMID: 33464539
- PMCID: PMC8119582
- DOI: 10.1007/s40122-020-00230-z
Cervical Proprioception Impairment in Neck Pain-Pathophysiology, Clinical Evaluation, and Management: A Narrative Review
Abstract
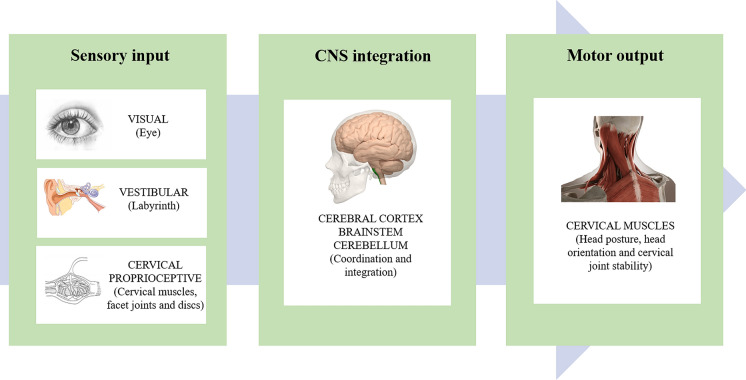
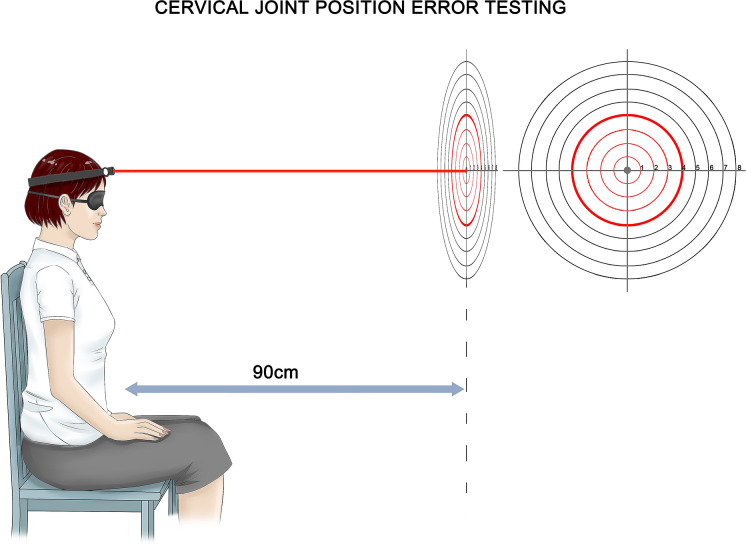
Neck pain is very common, but most of the causes are unknown, making diagnosis and treatment extremely challenging. Current studies have found that one of the main problems in patients with neck pain is the impairment of cervical proprioception, which subsequently leads to cervical sensorimotor control disturbances. Cervical spine has a very delicate proprioceptive system that plays a crucial role in controlling posture and balance. Cervical proprioceptive impairment in neck pain occurs through a variety of mechanisms. Experimental neck muscle pain induced by injection of hypertonic saline results in inhibition of the activation of painful muscle; chronic neck pain causes structural and functional impairment of cervical muscles; excessive activation of mechanoreceptors in degenerative cervical discs and facet joints produces a large number of erroneous sensory signals. Clinical examinations to assess the link between structural pathology and neck pain have been unsuccessful, opening the way for the development of function-based tests. To date, eight neck sensorimotor control tests have been reported to evaluate patients with chronic neck pain. Although some tests may involve different subsystems (such as oculomotor system and vestibular system), all tests measure sensorimotor control in the neck, and the most commonly used is cervical joint position error (JPE) test. Current studies support the effectiveness of exercises targeting different aspects of sensorimotor function, in particular retraining aimed at improving cervical proprioception and muscle coordination. Based on the available evidence, it is recommended that patients with neck pain should be assessed and managed for cervical proprioceptive impairment and sensorimotor control disturbances.
Keywords: Cervical joint position error; Cervical proprioception; Cervical proprioceptor; Cervical sensorimotor control; Neck pain; Pathophysiology; Rehabilitation.
Figures

Similar articles
-
Head and neck position sense.Sports Med. 2008;38(2):101-17. doi: 10.2165/00007256-200838020-00002. Sports Med. 2008. PMID: 18201114 Review.
-
Seven cervical sensorimotor control tests measure different skills in individuals with chronic idiopathic neck pain.Braz J Phys Ther. 2020 Jan-Feb;24(1):69-78. doi: 10.1016/j.bjpt.2018.10.013. Epub 2018 Nov 11. Braz J Phys Ther. 2020. PMID: 30446237 Free PMC article.
-
Cervical Joint Position Sense in Hypobaric Conditions: A Randomized Double-Blind Controlled Trial.Mil Med. 2017 Sep;182(9):e1969-e1975. doi: 10.7205/MILMED-D-16-00341. Mil Med. 2017. PMID: 28885964 Clinical Trial.
-
No Differences Between Individuals With Chronic Idiopathic Neck Pain and Asymptomatic Individuals on 7 Cervical Sensorimotor Control Tests: A Cross-sectional Study.J Orthop Sports Phys Ther. 2020 Jan;50(1):33-43. doi: 10.2519/jospt.2020.8846. J Orthop Sports Phys Ther. 2020. PMID: 31892290
-
Neck Pain: Do We Know Enough About the Sensorimotor Control System?Front Comput Neurosci. 2022 Jul 15;16:946514. doi: 10.3389/fncom.2022.946514. eCollection 2022. Front Comput Neurosci. 2022. PMID: 35910451 Free PMC article. Review.
Cited by
-
Comparison of balance and proprioception of the shoulder joint in girls with and without upper cross syndrome.BMC Musculoskelet Disord. 2024 Aug 2;25(1):618. doi: 10.1186/s12891-024-07552-5. BMC Musculoskelet Disord. 2024. PMID: 39095725 Free PMC article.
-
The relationship between cervical proprioception and balance in patients with fibromyalgia syndrome.Rheumatol Int. 2022 Feb;42(2):311-318. doi: 10.1007/s00296-021-05081-1. Epub 2022 Jan 8. Rheumatol Int. 2022. PMID: 34997841
-
Neck Muscle Vibration Alters Cerebellar Processing Associated with Motor Skill Acquisition of a Proprioceptive-Based Task.Brain Sci. 2023 Oct 4;13(10):1412. doi: 10.3390/brainsci13101412. Brain Sci. 2023. PMID: 37891781 Free PMC article.
-
Chronic Neck Pain Prevalence Before and After COVID-19 Restrictions and Its Relationship With Digital Device Screen Viewing: A Population Study.Ann Rehabil Med. 2024 Apr;48(2):124-134. doi: 10.5535/arm.230030. Epub 2024 Apr 22. Ann Rehabil Med. 2024. PMID: 38644637 Free PMC article.
-
Cervical Health Parameters in Car Drivers: Assessing the Influence of Driving on Neck Pain, Mobility, Proprioception and Craniovertebral Angle - A Cross-Sectional Study.J Multidiscip Healthc. 2024 May 2;17:2013-2020. doi: 10.2147/JMDH.S458364. eCollection 2024. J Multidiscip Healthc. 2024. PMID: 38716370 Free PMC article.
References
-
- Evans G. Identifying and treating the causes of neck pain. Med Clin North Am. 2014;98(3):645–661. - PubMed
-
- Cohen SP, Hooten WM. Advances in the diagnosis and management of neck pain. BMJ. 2017;358:j3221. - PubMed
-
- Treleaven J. Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control. Man Ther. 2008;13(1):2–11. - PubMed
-
- Treleaven J. Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control–Part 2: case studies. Man Ther. 2008;13(3):266–275. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
