

Does Keloid Histology Influence Recurrence?
- PMID: 33464754
- PMCID: PMC8273180
- DOI: 10.1097/DAD.0000000000001880
Does Keloid Histology Influence Recurrence?
Abstract
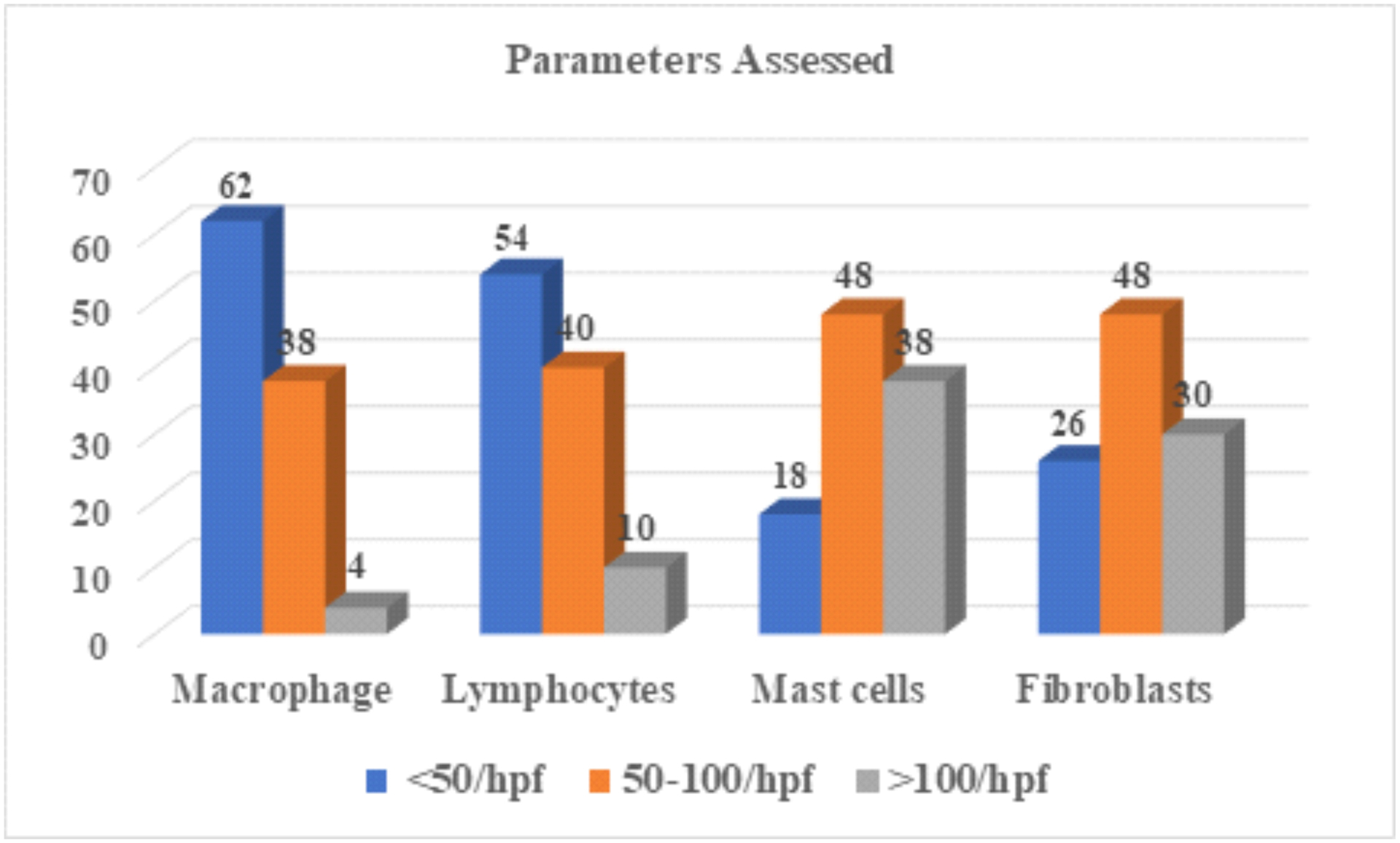
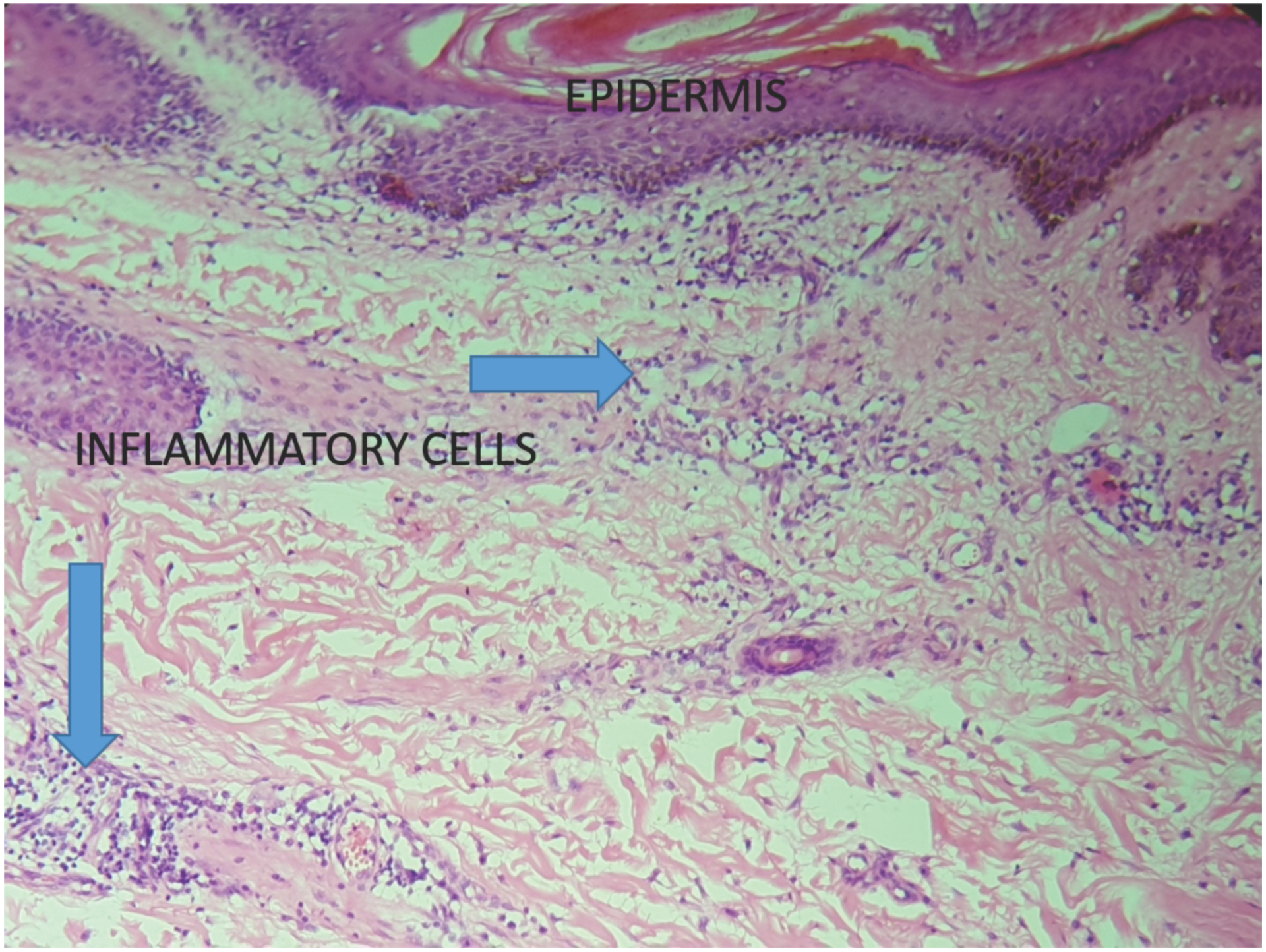
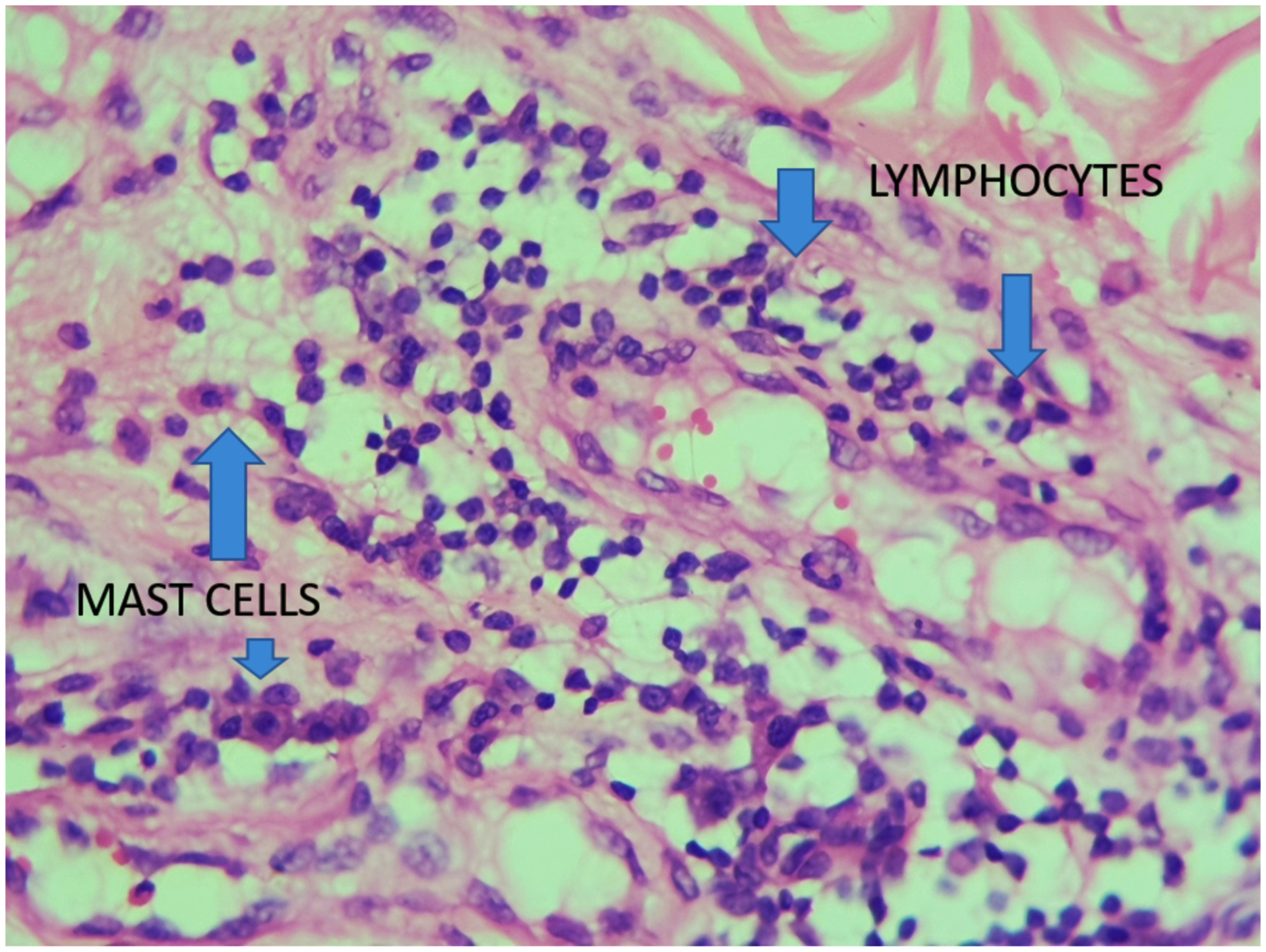
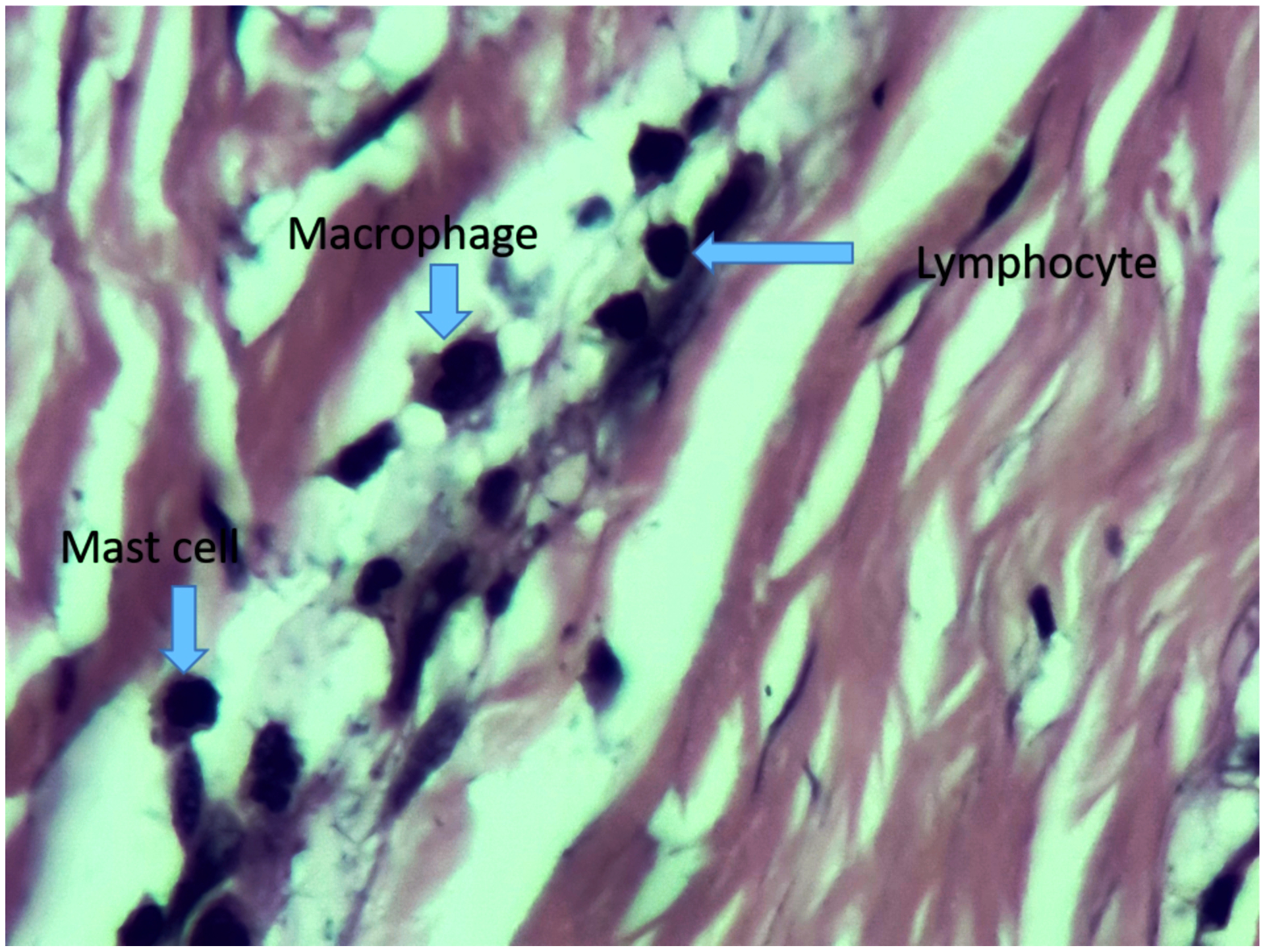
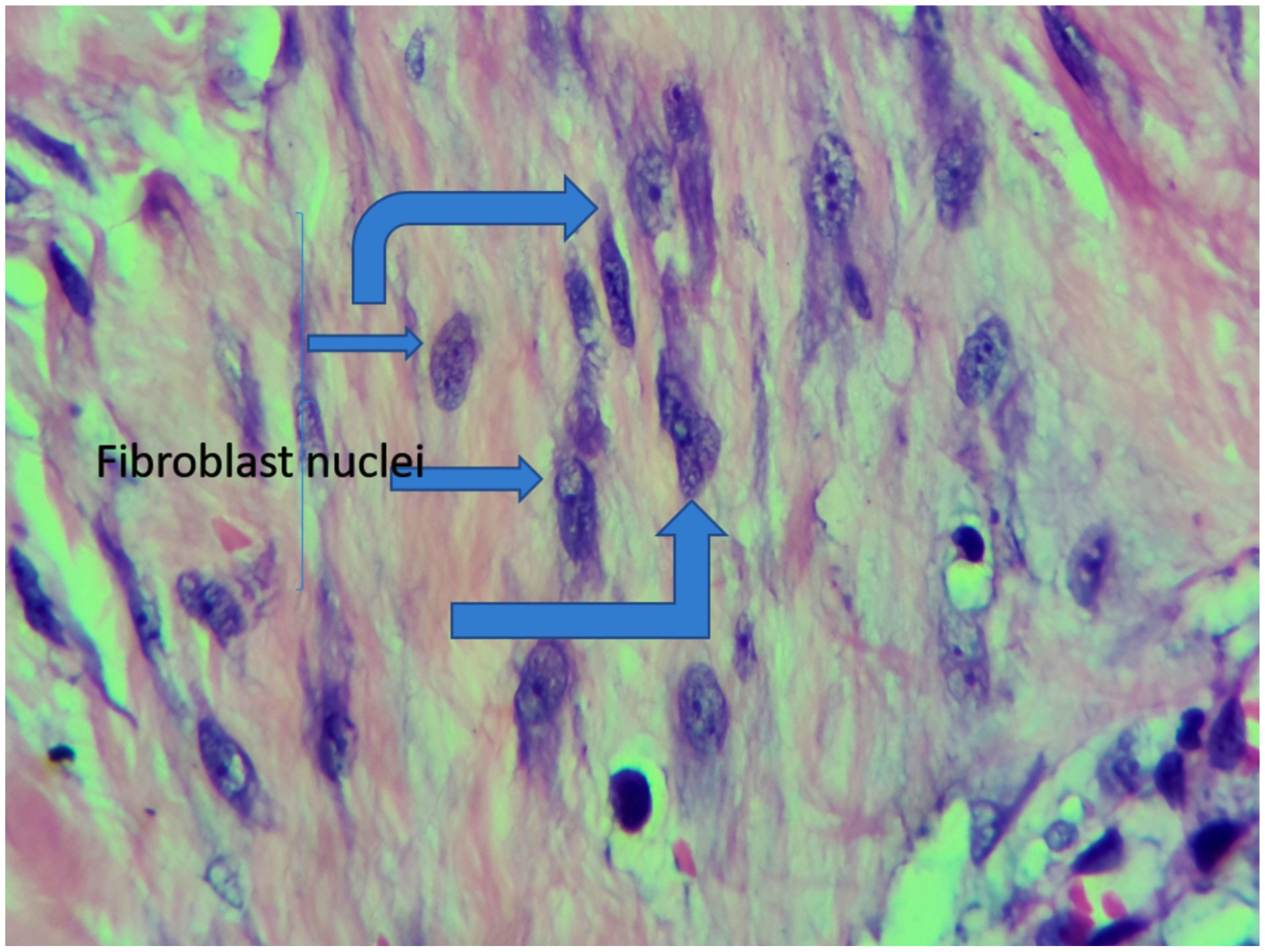
Keloids are fibroproliferative disorders characterized by high recurrence rates, with few factors known to influence the same. We conducted a study to determine whether keloid histology influences recurrence. This was a prospective longitudinal study to determine whether histopathological parameters of keloid influence recurrence. Patients with keloids managed by surgical excision were followed up at Kenyatta National Hospital between August 2018 and July 2020. The excised keloids were processed for histology using hematoxylin,/eosin, Masson, and trichrome stains. The slides were analyzed for inflammatory cells, fibroblasts, and capillary density using the hot spot technique and correlated to keloid recurrence. Postoperative follow-up was for a minimum of 1 year. A total of 90 patients with 104 keloids were recruited in the study. Overall keloid recurrence rate was 28.6%. There was a correlation between the absolute count of more than 50 per High power field of lymphocytes, fibroblasts, and macrophages with recurrence of the disease. The sensitivity and specificity for the above parameters were lymphocytes 48% and 81%, macrophages 57% and 83%, mast cells 32% and 33%, and fibroblasts 41% and 91%, respectively. There was no correlation between mast cells and vascularity status with recurrence. Routine histology should, therefore, be performed to determine these parameters. Close monitoring and second-line therapy should be considered for patients with elevated macrophages and/or lymphocytes so as to reduce the risk of recurrence.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Brissett A, Sherris DA Scar contractures, hypertrophic scars, and keloids. Facial Plast Surg 2001; 17:263–272. - PubMed
-
- Alexander,Petra P Hypertrophic scars and keloids-A review of their pathophysiology and therapeutic management, Dermatologic Surgery. March2009, 35 (2) 171–181 - PubMed
-
- Davis SA,Feldman SR,McMichael AJrvey. Management of keloids in the United States, 1990–2009: An analysis of the National Ambulatory Medical Care Survey. Dermatol Surg. 2013; 39(7):988–94(ISSN: 1524–4725) - PubMed
-
- Nast A, Eming S, Fluhr J, et al. German S2k guidelines for the therapy of pathological scars (hypertrophic scars and keloids). J Dtsch Dermatol Ges.. 2012October;10(10):747–62. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
