

Posture and gait in the early course of schizophrenia
- PMID: 33465166
- PMCID: PMC7815098
- DOI: 10.1371/journal.pone.0245661
Posture and gait in the early course of schizophrenia
Abstract
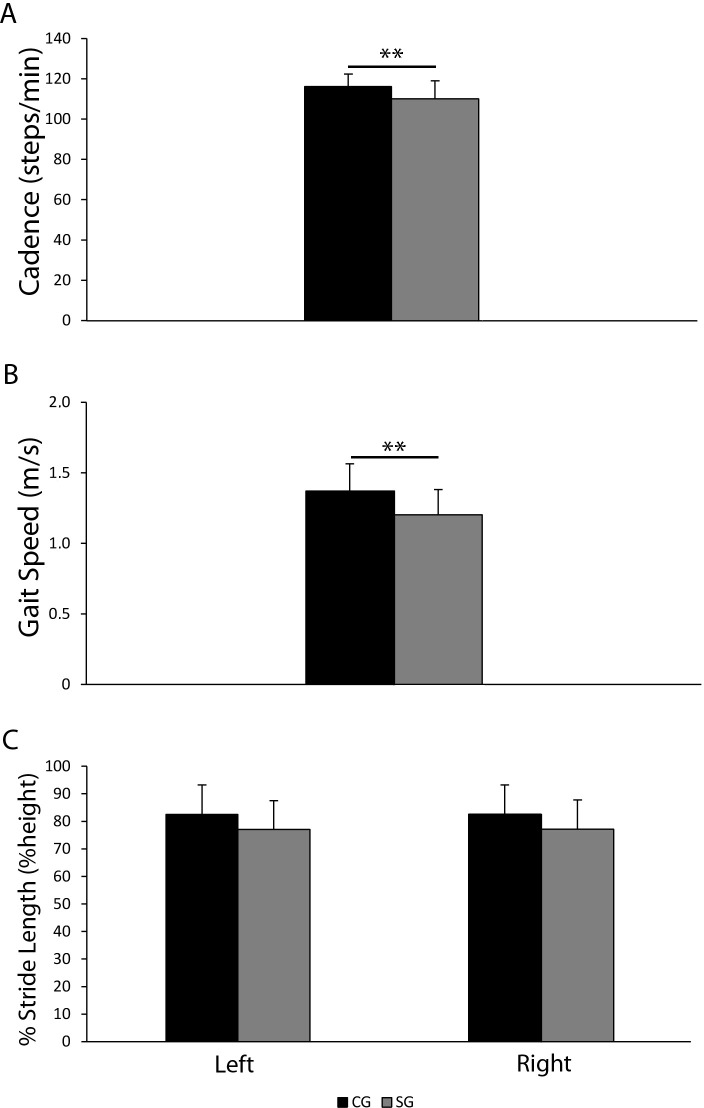
While correlations between postural stability deficits and schizophrenia are well documented, information on dynamic motor alterations in schizophrenia are still scarce, and no data on their onset are available yet. Therefore, the aim of this study was i) to measure gait pattern(s) in patients with schizophrenia; ii) to identify posture and gait alterations which could potentially be used as a predictive clinical tool of the onset of the disorder. Body composition, posture and gait parameters were assessed in a group of 30 patients with schizophrenia and compared to 25 healthy subjects. Sway area was significantly higher in the schizophrenia group compared to controls regardless of whether the participants were in eyes open or eyes closed condition. Gait cadence and speed were significantly lower in patients with schizophrenia, while stride length was similar. We concluded that the combination of an increased sway area (independent from eye closure) and a gait cadence reduction-in the presence of normal gait speed and stride length-might be considered peculiar postural and gait profile characteristic of early schizophrenia.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
