

Safety and Efficacy of PD-1/PD-L1 inhibitors combined with radiotherapy in patients with non-small-cell lung cancer: a systematic review and meta-analysis
- PMID: 33465302
- PMCID: PMC7926021
- DOI: 10.1002/cam4.3718
Safety and Efficacy of PD-1/PD-L1 inhibitors combined with radiotherapy in patients with non-small-cell lung cancer: a systematic review and meta-analysis
Abstract
Background: A combination of programmed cell death protein-1 (PD-1)/programmed cell death ligand-1 (PD-L1) inhibitors and radiotherapy (RT) is increasingly being used to treat non-small-cell lung cancer (NSCLC). However, the safety and efficacy of this approach remains controversial. We performed a systematic review and meta-analysis to summarize the related research.
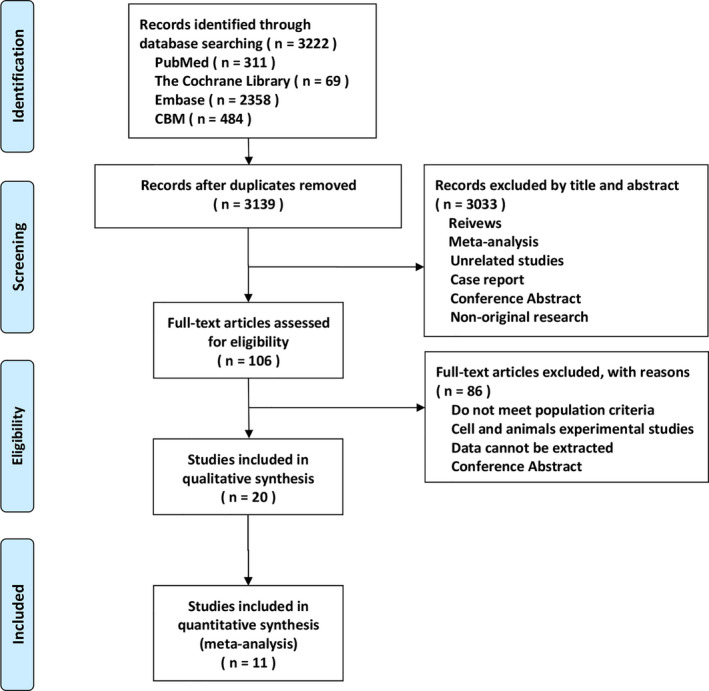
Methods: We searched the China Biology Medicine, EMBASE, Cochrane Library, and PubMed databases for all the relevant studies. The Stata software, version 12.0 was used for the meta-analysis.
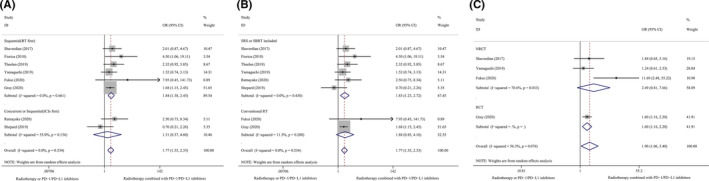
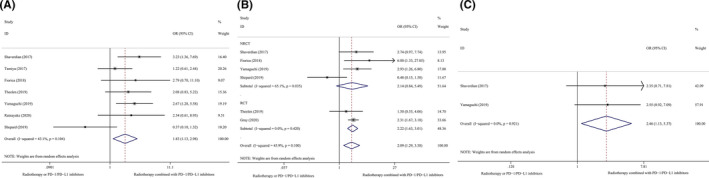
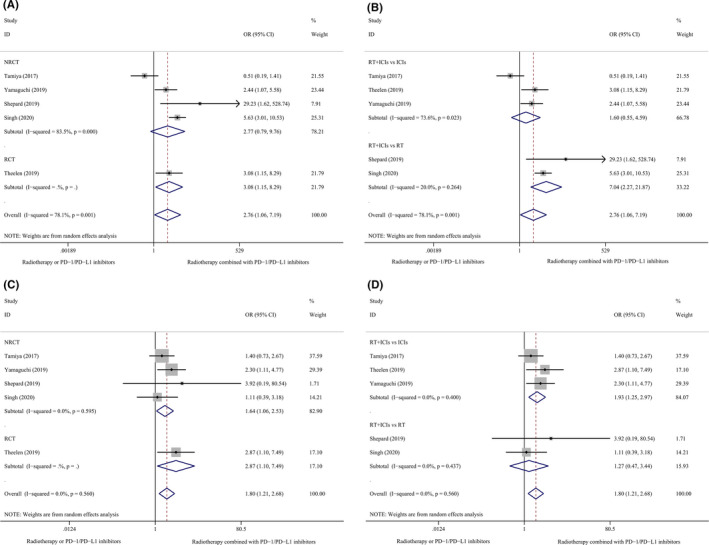
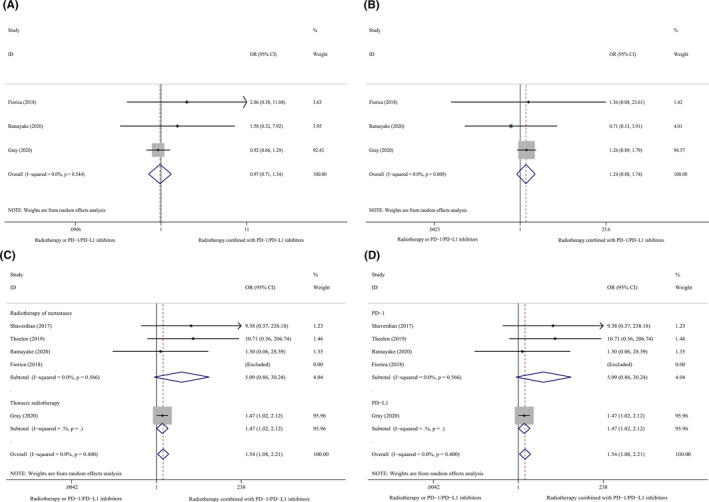
Results: The study included 20 clinical trials that enrolled 2027 patients with NSCLC. Compared with non-combination therapy, combination therapy using PD-1/PD-L1 inhibitors and RT was associated with prolonged overall survival (OS) (1-year OS: odds ratio [OR] 1.77, 95% confidence interval [CI] 1.35-2.33, p = 0.000; 2-year OS: OR 1.77, 95% CI 1.35-2.33, p = 0.000) and progression-free survival (PFS) (0.5-year PFS: OR 1.83, 95% CI 1.13-2.98, p = 0.014; 1-year PFS: OR 2.09, 95% CI 1.29-3.38, p = 0.003; 2-year PFS: OR 2.47, 95% CI 1.13-5.37, p = 0.023). Combination therapy also improved the objective response rate (OR 2.76, 95% CI 1.06-7.19, p = 0.038) and disease control rate (OR 1.80, 95% CI 1.21-2.68, p = 0.004). This meta-analysis showed that compared with non-combination therapy, combination therapy using PD-1/PD-L1 inhibitors and RT did not increase the serious adverse event rates (≥grade 3); however, this approach increased the rate of grade 1-2 immune-related or radiation pneumonitis. Subgroup analyses revealed that the sequence of PD-1/PD-L1 inhibitors followed RT outperformed in which concurrent PD-1/PD-L1 inhibitor and RT followed PD-1/PD-L1 inhibitor. Combination of stereotactic body RT or stereotactic radiosurgery with PD-1/PD-L1 inhibitors may be more effective than a combination of conventional RT with PD-1/PD-L1 inhibitors in patients with advanced NSCLC.
Conclusion: Combination therapy using PD-1/PD-L1 inhibitors and RT may improve OS, PFS, and tumor response rates without an increase in serious adverse events in patients with advanced NSCLC. However, combination therapy was shown to increase the incidence of mild pneumonitis.
Keywords: combined radio-immunotherapy; meta-analysis; non-small-cell lung cancer; programmed cell death protein-1/programmed cell death ligand-1 inhibitors; radiotherapy; systematic review.
© 2021 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors have no conflict of interest.
Figures
Similar articles
-
Effectivity and safety of PD-1/PD-L1 inhibitors for different level of PD-L1-positive, advanced NSCLC: A meta-analysis of 4939 patients from randomized controlled trials.Int Immunopharmacol. 2020 Jul;84:106452. doi: 10.1016/j.intimp.2020.106452. Epub 2020 Apr 24. Int Immunopharmacol. 2020. PMID: 32339922
-
Efficacy and safety of first-line PD-1/PD-L1 inhibitor in combination with CTLA-4 inhibitor in the treatment of patients with advanced non-small cell lung cancer: a systemic review and meta-analysis.Front Immunol. 2025 Feb 6;16:1515027. doi: 10.3389/fimmu.2025.1515027. eCollection 2025. Front Immunol. 2025. PMID: 39981238 Free PMC article.
-
Comparative efficacy and safety of PD-1/PD-L1 Inhibitors versus platinum-based chemotherapy for the first-line treatment of advanced non-small cell lung cancer: a meta analysis of randomized controlled trials.Pharmacol Res. 2020 Oct;160:105194. doi: 10.1016/j.phrs.2020.105194. Epub 2020 Sep 13. Pharmacol Res. 2020. PMID: 32937178
-
The relative and absolute benefit of programmed death receptor-1 vs programmed death ligand 1 therapy in advanced non-small-cell lung cancer: A systematic review and meta-analysis.Int Immunopharmacol. 2020 Oct;87:106852. doi: 10.1016/j.intimp.2020.106852. Epub 2020 Aug 3. Int Immunopharmacol. 2020. PMID: 32759049
-
SBRT combined with PD-1/PD-L1 inhibitors in NSCLC treatment: a focus on the mechanisms, advances, and future challenges.J Hematol Oncol. 2020 Jul 28;13(1):105. doi: 10.1186/s13045-020-00940-z. J Hematol Oncol. 2020. PMID: 32723363 Free PMC article. Review.
Cited by
-
Dostarlimab an Inhibitor of PD-1/PD-L1: A New Paradigm for the Treatment of Cancer.Medicina (Kaunas). 2022 Nov 1;58(11):1572. doi: 10.3390/medicina58111572. Medicina (Kaunas). 2022. PMID: 36363529 Free PMC article. Review.
-
Late combination of transarterial chemoembolization with apatinib and camrelizumab for unresectable hepatocellular carcinoma is superior to early combination.BMC Cancer. 2022 Mar 27;22(1):335. doi: 10.1186/s12885-022-09451-1. BMC Cancer. 2022. PMID: 35346114 Free PMC article.
-
Carbon ion irradiation combined with PD-1 inhibitor trigger abscopal effect in Lewis lung cancer via a threshold dose.J Cancer. 2024 Feb 25;15(8):2245-2259. doi: 10.7150/jca.91559. eCollection 2024. J Cancer. 2024. PMID: 38495488 Free PMC article.
-
A retrospective study of the efficacy and safety of immune checkpoint inhibitors combined with chemotherapy for the treatment of SMARCA4-deficient thoracic tumors.Transl Lung Cancer Res. 2024 Dec 31;13(12):3460-3472. doi: 10.21037/tlcr-24-691. Epub 2024 Dec 27. Transl Lung Cancer Res. 2024. PMID: 39830761 Free PMC article.
-
PD-1 Impairs CD8+ T Cell Granzyme B Production in Aged Mice during Acute Viral Respiratory Infection.Immunohorizons. 2023 Nov 1;7(11):771-787. doi: 10.4049/immunohorizons.2300094. Immunohorizons. 2023. PMID: 38015461 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7‐30. - PubMed
-
- Su S, Li T, Lu B, et al. Three‐dimensional radiation therapy to the primary tumor with concurrent chemotherapy in patients with stage IV non‐small cell lung cancer: results of a multicenter phase 2 study from PPRA‐RTOG, China. Int J Radiat Oncol Biol Phys. 2015;93(4):769‐777. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
