

Evaluating the Impact of Stopping Chronic Therapies after Modulator Drug Therapy in Cystic Fibrosis: The SIMPLIFY Clinical Trial Study Design
- PMID: 33465316
- PMCID: PMC8513667
- DOI: 10.1513/AnnalsATS.202010-1336SD
Evaluating the Impact of Stopping Chronic Therapies after Modulator Drug Therapy in Cystic Fibrosis: The SIMPLIFY Clinical Trial Study Design
Abstract
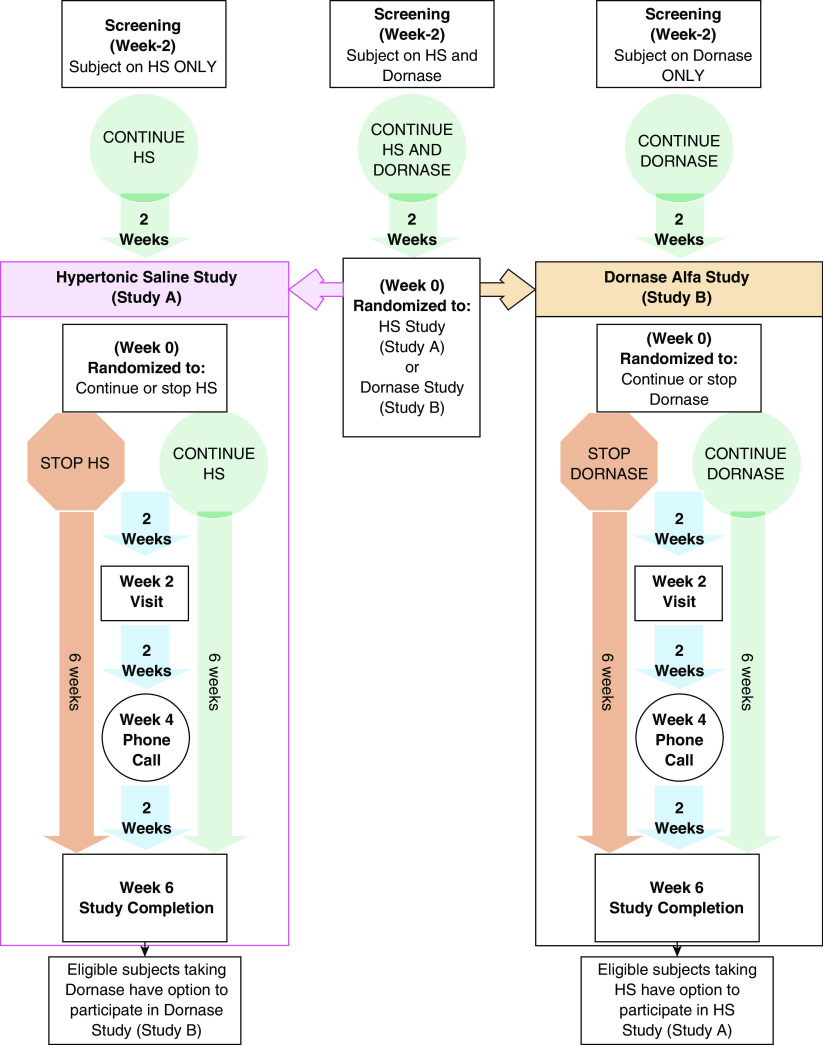
The care for individuals with cystic fibrosis (CF) with at least one F508del mutation will greatly change as a result of the unparalleled clinical benefits observed with the new triple-combination CFTR (CF transmembrane regulator)-modulator therapy elexacaftor/tezacaftor/ivacaftor (ETI). Incorporating ETI into the standard of care creates new motivation and opportunity to consider reductions in overall treatment burden and evaluate whether other chronic medications can now be safely discontinued without loss of clinical benefit. SIMPLIFY is a master protocol poised to test the impact of discontinuing versus continuing two commonly used chronic therapies in people with CF who are at least 12 years of age or older and stable on ETI therapy. The protocol is composed of two concurrent randomized controlled trials designed to evaluate the independent short-term effects of discontinuing hypertonic saline or dornase alfa, enabling individuals on both therapies to participate in one or both trials. The primary objective for each trial is to determine whether discontinuing treatment is noninferior to continuing treatment after establishment of ETI, as measured by the 6-week absolute change in the percent-predicted forced expiratory volume in 1 second. Developing this study required a balance between ideal study-design principles and feasibility. SIMPLIFY will be the largest multicenter, randomized, controlled medication-withdrawal study in CF. This study is uniquely positioned to provide timely evidence on whether the daily treatment burden can be reduced among individuals on CFTR-modulator therapy. Clinical trial registered with www.clinicaltrials.gov (NCT04378153).
Keywords: CFTR modulators; noninferiority trial; treatment burden.
Figures
References
-
- Heijerman HGM, McKone EF, Downey DG, Van Braeckel E, Rowe SM, Tullis E, et al. VX17-445-103 Trial Group. Efficacy and safety of the elexacaftor plus tezacaftor plus ivacaftor combination regimen in people with cystic fibrosis homozygous for the F508del mutation: a double-blind, randomised, phase 3 trial. Lancet. 2019;394:1940–1948. - PMC - PubMed
-
- Sawicki GS, McKone EF, Pasta DJ, Millar SJ, Wagener JS, Johnson CA, et al. Sustained benefit from ivacaftor demonstrated by combining clinical trial and cystic fibrosis patient registry data. Am J Respir Crit Care Med. 2015;192:836–842. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
