

Avapritinib in unresectable or metastatic PDGFRA D842V-mutant gastrointestinal stromal tumours: Long-term efficacy and safety data from the NAVIGATOR phase I trial
- PMID: 33465704
- PMCID: PMC9518931
- DOI: 10.1016/j.ejca.2020.12.008
Avapritinib in unresectable or metastatic PDGFRA D842V-mutant gastrointestinal stromal tumours: Long-term efficacy and safety data from the NAVIGATOR phase I trial
Abstract
Background: PDGFRA D842V mutations occur in 5-10% of gastrointestinal stromal tumours (GISTs), and previously approved tyrosine kinase inhibitors (TKIs) are inactive against this mutation. Consequently, patients have a poor prognosis. We present an updated analysis of avapritinib efficacy and long-term safety in this patient population.
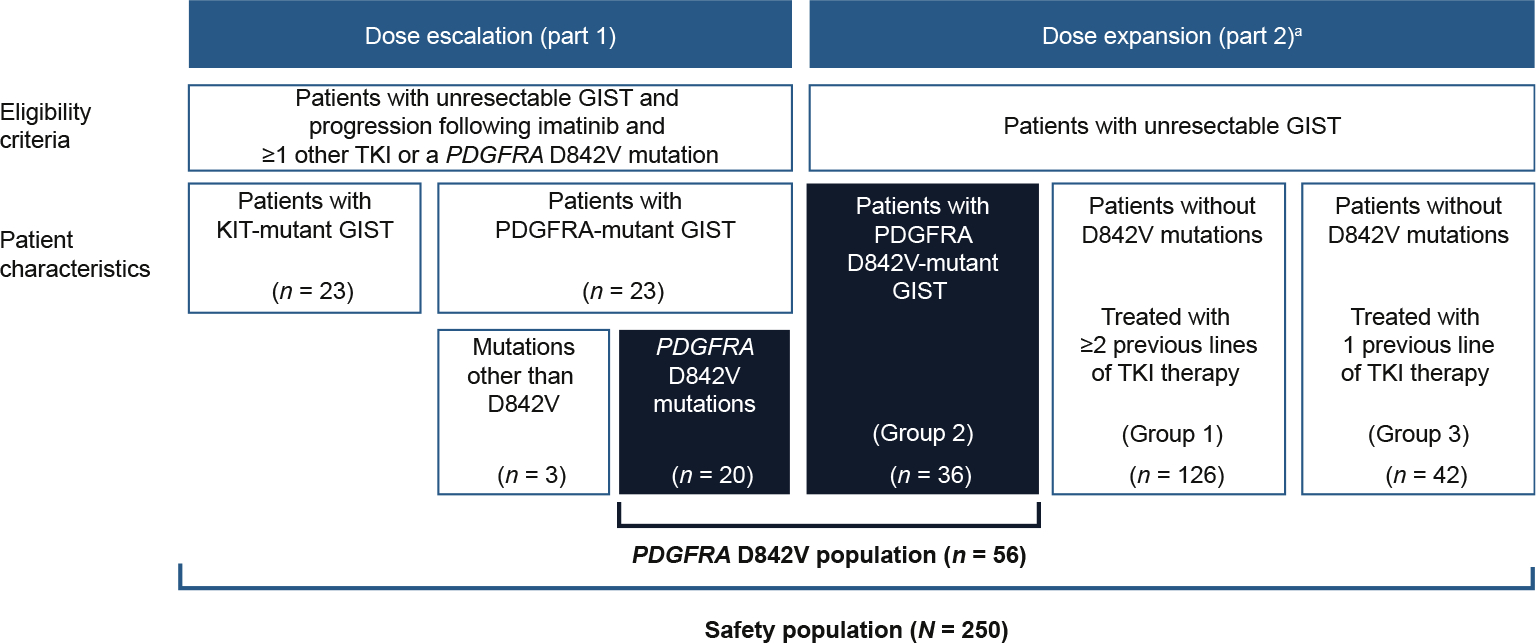
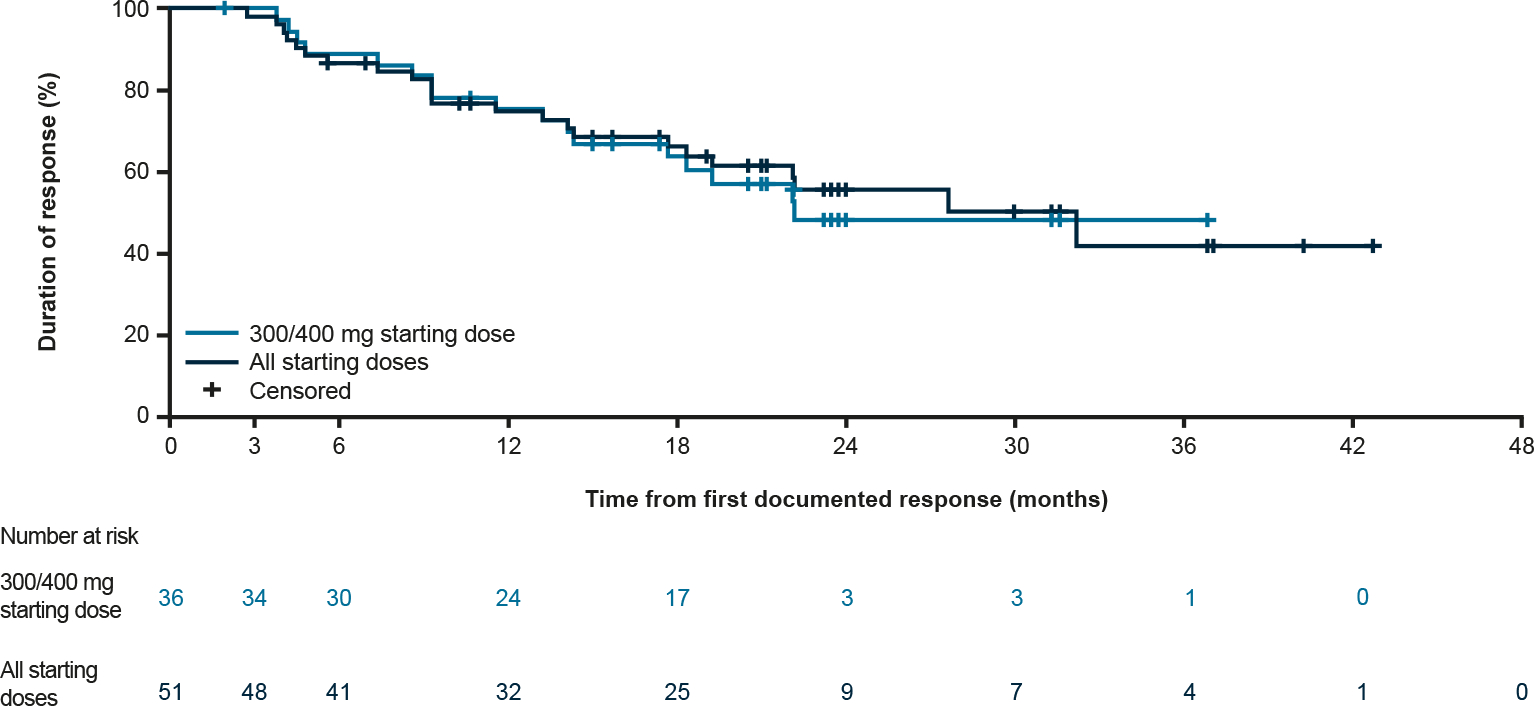
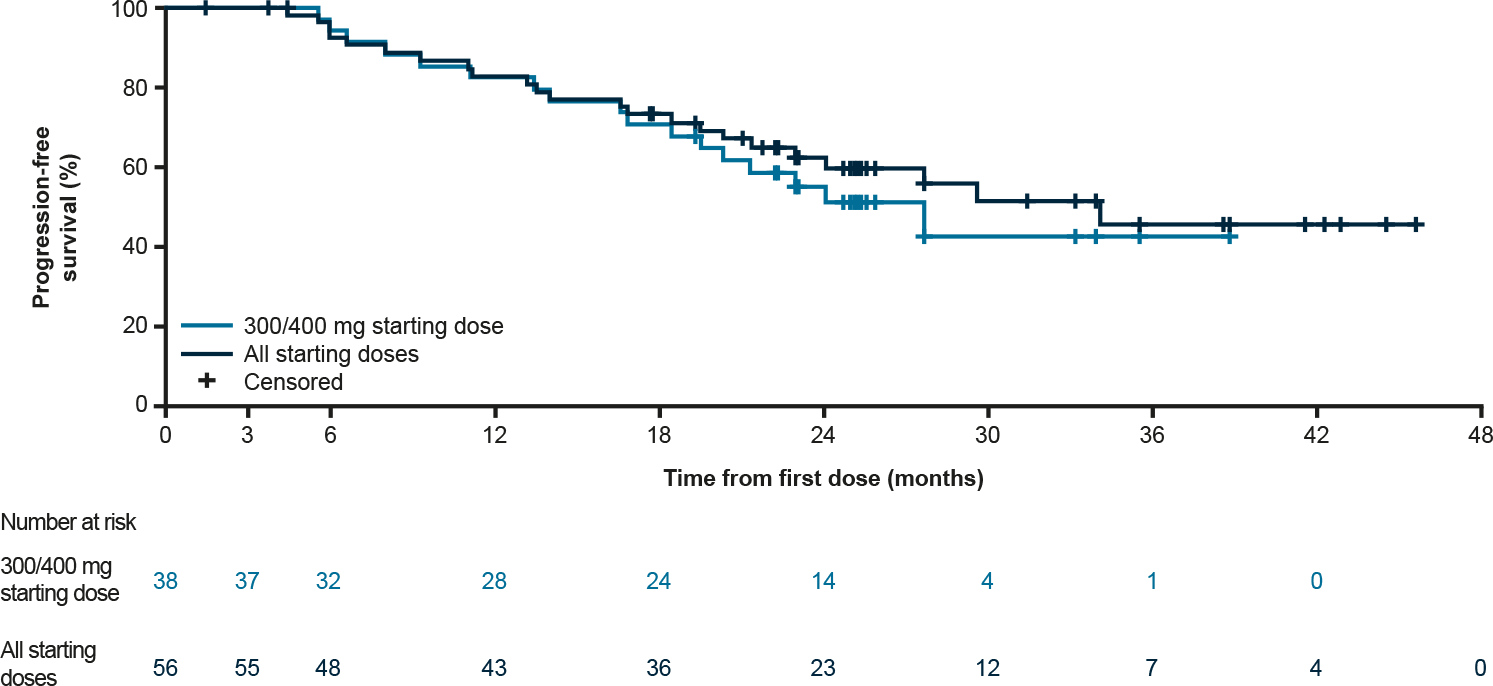
Methods: NAVIGATOR (NCT02508532), a two-part, open-label, dose-escalation/dose-expansion phase I study, enrolled adult patients with unresectable GISTs. Patients with PDGFRA D842V-mutant GIST were a prespecified subgroup within the overall safety population, which included patients who received ≥1 avapritinib dose. Primary end-points were overall response rate (ORR) and avapritinib safety profile. Secondary end-points were clinical benefit rate (CBR), duration of response (DOR) and progression-free survival (PFS). Overall survival (OS) was an exploratory end-point.
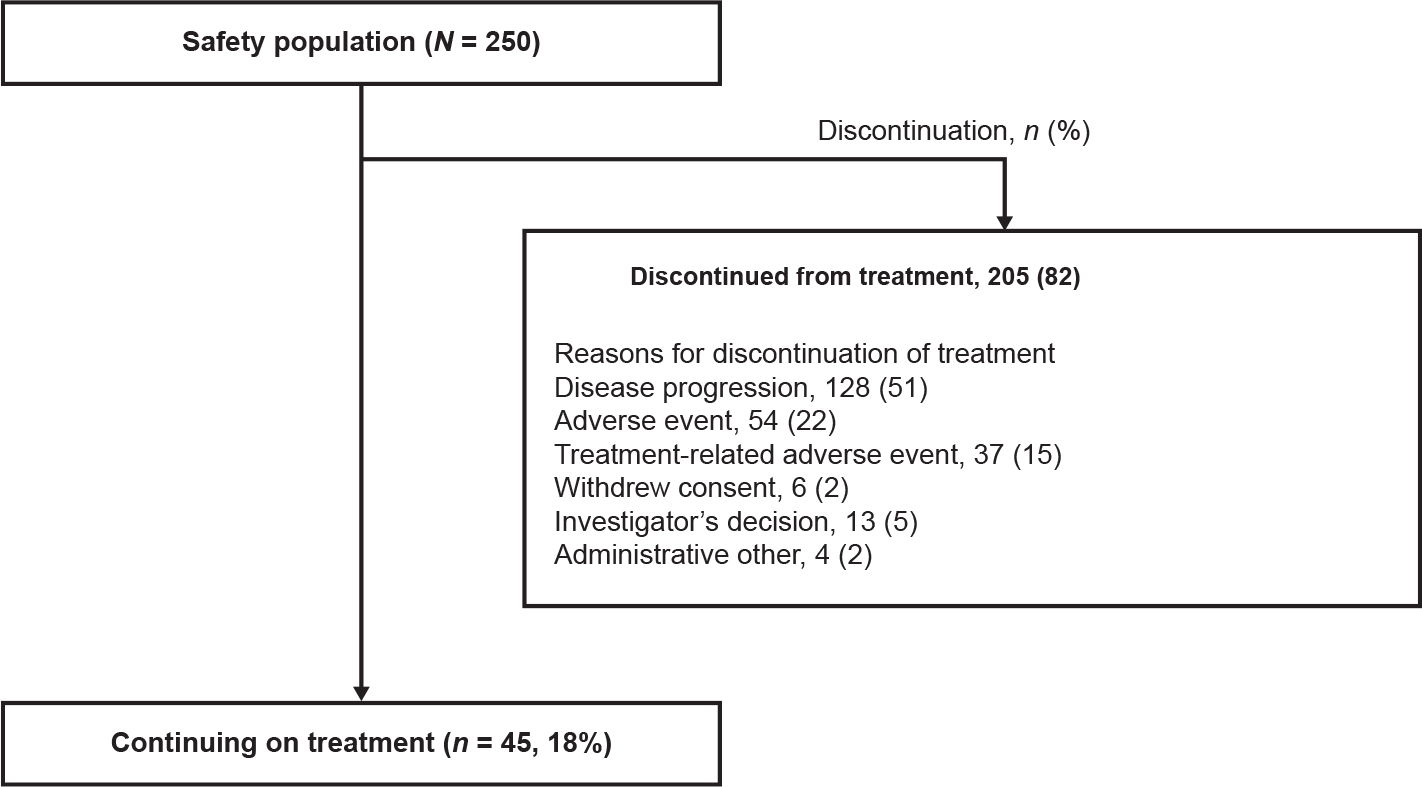
Results: Between 7 October 2015 and 9 March 2020, 250 patients enrolled in the safety population; 56 patients were included in the PDGFRA D842V population, 11 were TKI-naïve. At data cut-off, median follow-up was 27.5 months. Safety profile was comparable between the overall safety and PDGFRA D842V populations. In the PDGFRA D842V population, the most frequent adverse events were nausea (38 [68%] patients) and diarrhoea (37 [66%]), and cognitive effects occurred in 32 (57%) patients. The ORR was 91% (51/56 patients). The CBR was 98% (55/56 patients). The median DOR was 27.6 months (95% confidence interval [CI]: 17.6-not reached [NR]); median PFS was 34.0 months (95% CI: 22.9-NR). Median OS was not reached.
Conclusion: Targeting PDGFRA D842V-mutant GIST with avapritinib resulted in an unprecedented, durable clinical benefit, with a manageable safety profile. Avapritinib should be considered as first-line therapy for these patients.
Keywords: Avapritinib; Gastrointestinal stromal tumours; PDGFRA; Phase 1.
Copyright © 2020 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Conflict of interest statement Dr Jones reported receiving grants from MSD; and personal fees from Adaptimmune, Athenex, Blueprint Medicines Corporation, Clinigen, Eisai, Eli Lilly, Epizyme, Daichii Sankyo, Deciphera Pharmaceuticals, Helsinn, Immunedesign, Merck, PharmaMar, Tracon and UptoDate outside the submitted work. Dr Serrano reported receiving other support from Bayer, Blueprint Medicines Corporation, Deciphera Pharmaceuticals, Eli Lilly, Novartis, Pfizer and PharmaMar; and grants from Bayer, Deciphera Pharmaceuticals and Pfizer outside the submitted work. Dr von Mehren reported receiving other support from Blueprint Medicines Corporation during the conduct of the study; and other support from Arog Pharmaceuticals, Deciphera Pharmaceuticals, Exelixis and Novartis outside the submitted work. Dr George reported receiving research support to her institution from Ariad, Bayer, Blueprint Medicines Corporation, Daiichi Sankyo, Deciphera Pharmaceuticals, Novartis and Pfizer; and advisory board/consulting fees from AstraZeneca, Blueprint Medicines Corporation, Daiichi Sankyo, Deciphera Pharmaceuticals and Eli Lilly. Dr Heinrich reported receiving grants and personal fees from Blueprint Medicines Corporation; and personal fees and other support from Molecular MD during the conduct of the study; personal fees and other from Novartis; and grants and personal fees from Deciphera Pharmaceuticals outside the submitted work. Dr Heinrich also has a patent “Treatment of Gastrointestinal Stromal Tumors” licenced to Novartis, and a patent “Activating Mutations of PDGFRA” issued. Dr Kang reported receiving personal fees from ALX Oncology, Amgen, Bristol Myers Squibb, Daehwa Pharmaceutical, MacroGenics, Novartis, Surface Oncology and Zymeworks outside the submitted work. Dr Schöffski reported receiving personal fees from Deciphera Pharmaceuticals; other support from Adaptimmune, Blueprint Medicines Corporation, Deciphera Pharmaceuticals, Exelixis, Eisai, Eli Lilly, Ellipses Pharma, Genmab, Intellisphere, Loxo Oncology, Merck, Plexxikon, Servier and Transgene; and grants from Ipsen and MSD outside the submitted work. Dr Cassier reported receiving personal fees from Blueprint Medicines Corporation during the conduct of the study; other support from AbbVie, Bayer, Bristol Myers Squibb, Eli Lilly, GlaxoSmithKline, Janssen, Merck Serono, MSD, Novartis and Roche/Genentech; personal fees from Amgen, Bristol Myers Squibb, MSD, Novartis and Roche/Genentech; non-financial support from MSD and Novartis; and grants from Novartis outside the submitted work. Dr Mir reported receiving consulting fees from Eli Lilly, Janssen, Lundbeck, Pfizer, Roche, Servier and Vifor Pharma; and owns stock options from Amplitude Surgical, Transgene and Ipsen. Dr Chawla reported receiving funding from ADI, Amgen, GlaxoSmithKline, Ignyta, Immix Bopharma, Inhibrx, Janssen, Karyopharm Therapeutics, Roche, SARC and Tracon outside the submitted work. Dr Eskens has nothing to disclose. Dr Rutkowski reported receiving personal fees from Blueprint Medicines Corporation, Bristol Myers Squibb, Merck, MSD, Novartis, Pierre Fabre, Pfizer, Roche and Sanofi outside the submitted work. Dr Tap reported receiving other support from Blueprint Medicines Corporation during the conduct of the study; receiving personal fees from Agios Pharmaceuticals, Blueprint Medicines Corporation, Daiichi Sankyo, Deciphera Pharmaceuticals, Eli Lilly, EMD Serono, Eisai, GlaxoSmithKline, Janssen, Immune Design, Loxo Oncology and NanoCarrier outside the submitted work; having a patent Companion Diagnostic for CDK4 inhibitors – 14/854,329 pending to MSKCC/SKI; attending scientific advisory boards for Atropos Therapeutics and Certis Oncology Solutions; being a consultant for Daiichi Sankyo; having stock ownership in Atropos Therapeutics and Daiichi Sankyo; and having involvement in an FDA ODAC meeting for pexidartinib. Dr Zhou is a former employee of Blueprint Medicines Corporation. Dr Roche reported receiving other support from Epizyme outside the submitted work; and being a current employee and shareholder of Blueprint Medicines Corporation. Dr Bauer reported receiving grants from Blueprint Medicines Corporation, Incyte and Novartis; personal fees from Bayer, Blueprint Medicines Corporation, Deciphera Pharmaceuticals, Exelixis and Novartis during the conduct of the study; and personal fees from ADC Therapeutics, Daiichi Sankyo, Eli Lilly, Exelixis, Janssen-Cilag, Nanobiotix, PharmaMar and Plexxikon outside the submitted work.
Figures


Comment in
-
Circulating tumour DNA sequencing reveal mechanisms of resistance to BRAF-targeted therapies in BRAF-mutated gastrointestinal stromal tumour.Eur J Cancer. 2023 Jan;179:25-27. doi: 10.1016/j.ejca.2022.10.018. Epub 2022 Nov 1. Eur J Cancer. 2023. PMID: 36470024 No abstract available.
References
-
- Heinrich MC, Corless CL, Duensing A, et al. PDGFRA activating mutations in gastrointestinal stromal tumors. Science 2003;299:708–10. - PubMed
-
- Corless CL, Schroeder A, Griffith D, et al. PDGFRA mutations in gastrointestinal stromal tumors: frequency, spectrum and in vitro sensitivity to imatinib. J Clin Oncol 2005;23:5357–64. - PubMed
-
- Hirota S, Ohashi A, Nishida T, et al. Gain-of-function mutations of platelet-derived growth factor receptor alpha gene in gastrointestinal stromal tumors. Gastroenterology 2003;125:660–7. - PubMed
-
- Roubaud G, Kind M, Coindre JM, et al. Clinical activity of sorafenib in patients with advanced gastrointestinal stromal tumor bearing PDGFRA exon 18 mutation: a case series. Ann Oncol 2012;23:804–5. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
