

Uveitis as an Open Window to Systemic Inflammatory Diseases
- PMID: 33466638
- PMCID: PMC7828680
- DOI: 10.3390/jcm10020281
Uveitis as an Open Window to Systemic Inflammatory Diseases
Abstract
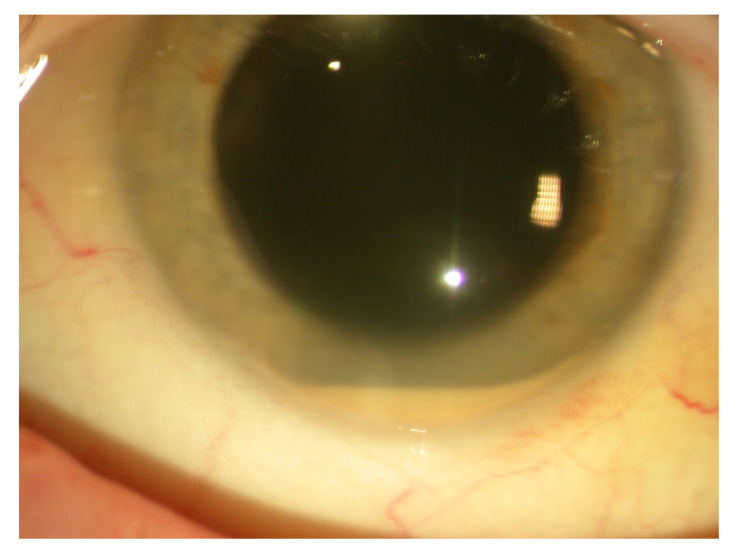
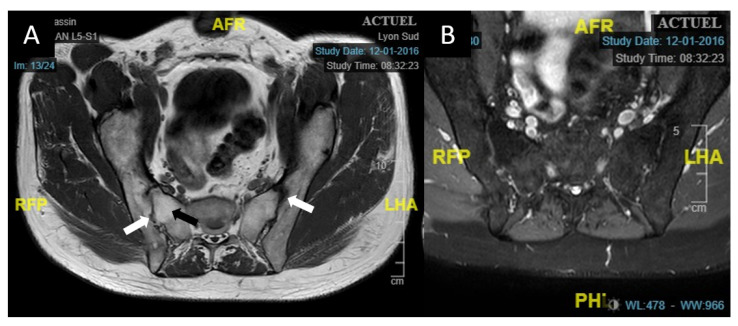
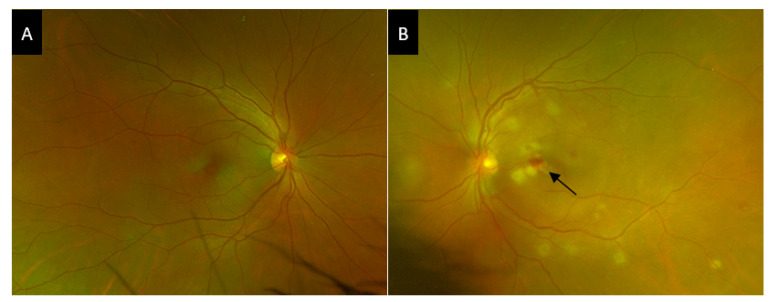
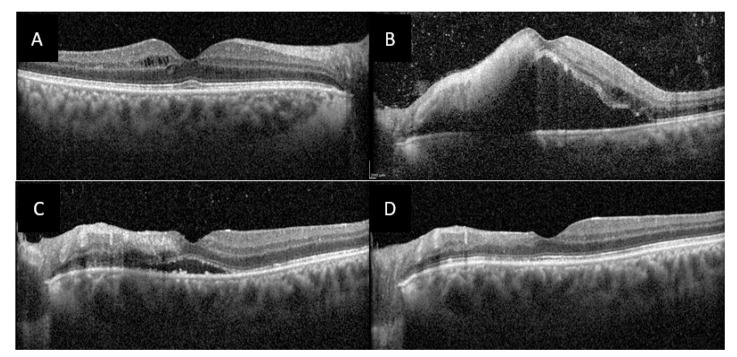
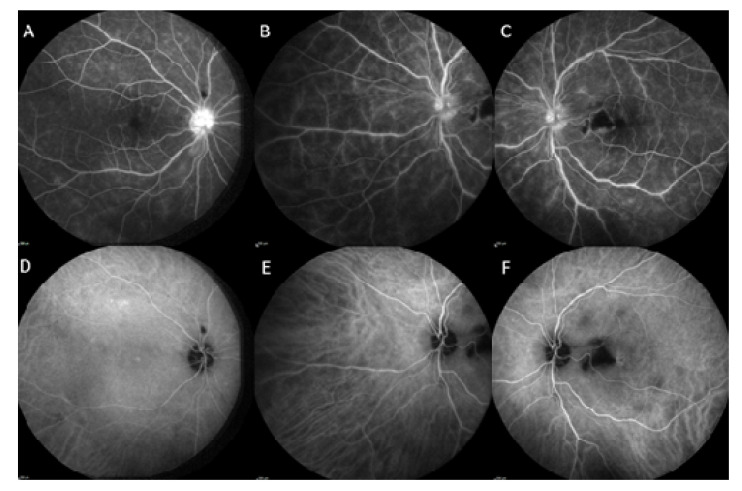
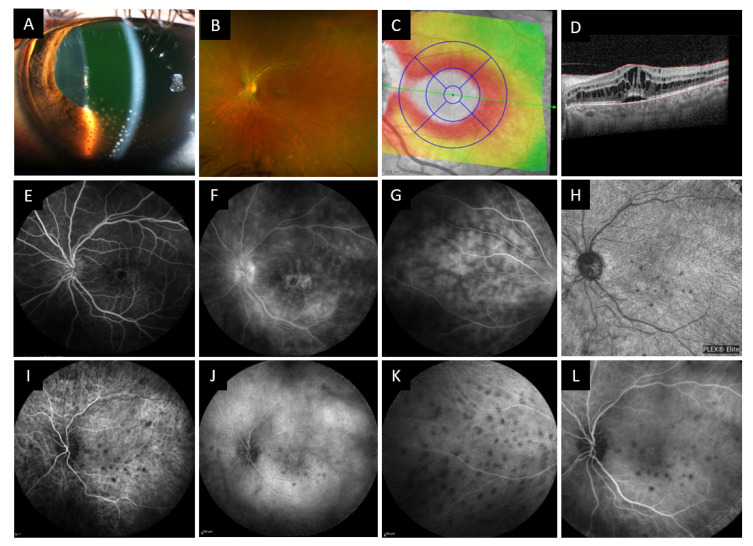
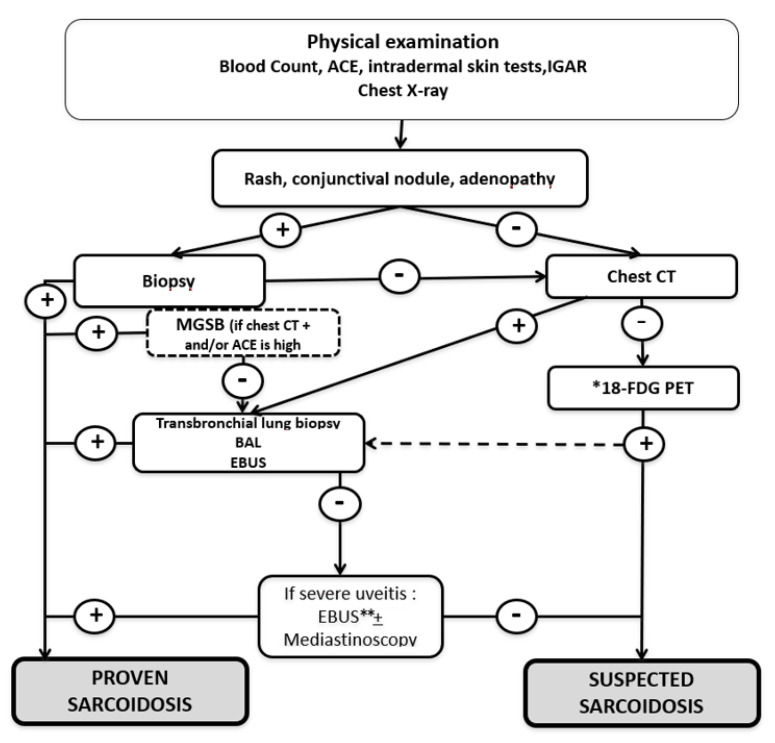
Spondyloarthritis (Spa), Behçet's disease (BD) and sarcoidosis are major systemic inflammatory diseases worldwide. They are all multisystem pathologies and share a possible ocular involvement, especially uveitis. We hereby describe selected cases who were referred by ophthalmologists to our internal medicine department for unexplained uveitis. Physical examination and/or the use of laboratory and imaging investigations allowed to make a diagnosis of a systemic inflammatory disease in a large proportion of patients. In our tertiary referral center, 75 patients have been diagnosed with Spa (n = 20), BD (n = 9), or sarcoidosis (n = 46) in the last two years. There was a significant delay in the diagnosis of Spa-associated uveitis. Screening strategies using Human Leukocyte Antigen (HLA)-B27 determination and sacroiliac magnetic resonance imaging in patients suffering from chronic low back pain and/or psoriasis helped in the diagnosis. BD's uveitis affects young people from both sexes and all origins and usually presents with panuveitis and retinal vasculitis. The high proportion of sarcoidosis in our population is explained by the use of chest computed tomography (CT) and 18F-fluorodeoxyglucose positron emission tomography CT that helped to identify smaller hilar or mediastinal involvement and allowed to further investigate those patients, especially in the elderly. Our results confirm how in these sight- and potentially life-threatening diseases a prompt diagnosis is mandatory and benefits from a multidisciplinary approach.
Keywords: Behçet’s disease; HLA-B27 associated uveitis; sarcoidosis; spondyloarthritis; uveitis.
Conflict of interest statement
Laurent Kodjikian declared conflicts of interest from Abbvie, Allergan, Bayer, Novartis, Roche, Théa. Other authors declare no conflict of interests.
Figures
References
-
- Dick A.D., Rosenbaum J.T., Al-Dhibi H.A., Belfort R., Brézin A.P., Chee S.-P., Davis J.L., Ramanan A.V., Sonoda K.-H., Carreño E., et al. Guidance on Noncorticosteroid Systemic Immunomodulatory Therapy in Noninfectious Uveitis. Ophthalmology. 2018;125:757–773. doi: 10.1016/j.ophtha.2017.11.017. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
