

Gait Recovery with an Overground Powered Exoskeleton: A Randomized Controlled Trial on Subacute Stroke Subjects
- PMID: 33466749
- PMCID: PMC7830339
- DOI: 10.3390/brainsci11010104
Gait Recovery with an Overground Powered Exoskeleton: A Randomized Controlled Trial on Subacute Stroke Subjects
Abstract
Background: Overground Robot-Assisted Gait Training (o-RAGT) provides intensive gait rehabilitation. This study investigated the efficacy of o-RAGT in subacute stroke subjects, compared to conventional gait training.
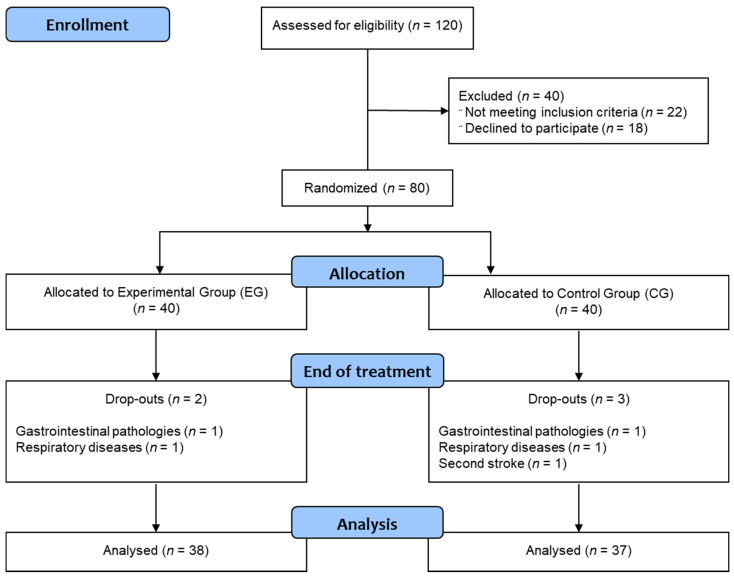
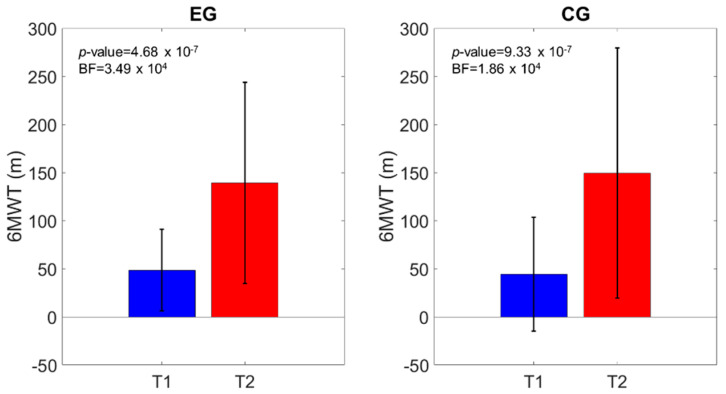
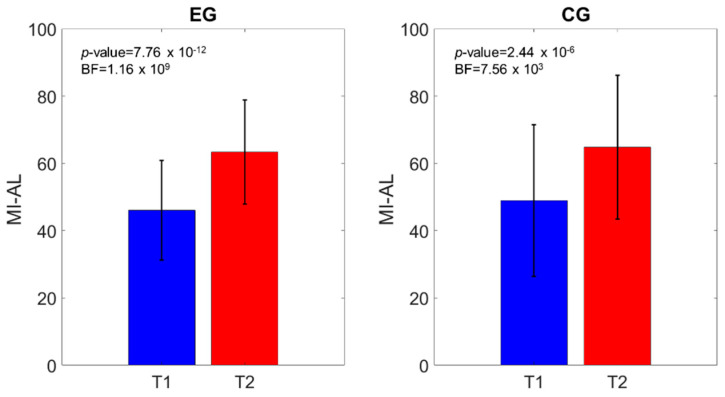
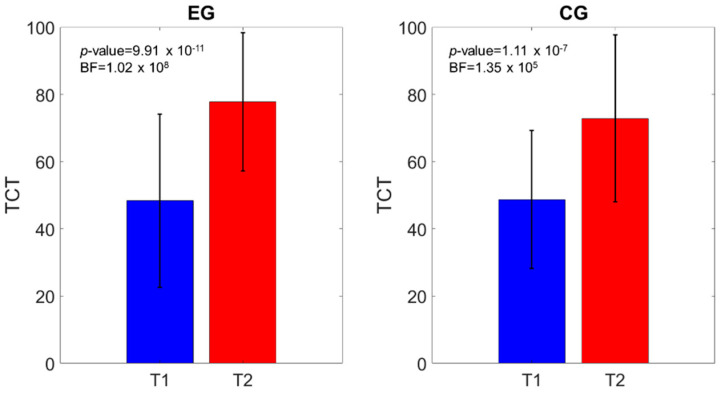
Methods: A multicenter randomized controlled trial was conducted on 75 subacute stroke subjects (38 in the Experimental Group (EG) and 37 in the Control Group (CG)). Both groups received 15 sessions of gait training (5 sessions/week for 60 min) and daily conventional rehabilitation. The subjects were assessed at the beginning (T1) and end (T2) of the training period with the primary outcome of a 6 Minutes Walking Test (6MWT), the Modified Ashworth Scale of the Affected lower Limb (MAS-AL), the Motricity Index of the Affected lower Limb (MI-AL), the Trunk Control Test (TCT), Functional Ambulation Classification (FAC), a 10 Meters Walking Test (10MWT), the modified Barthel Index (mBI), and the Walking Handicap Scale (WHS).
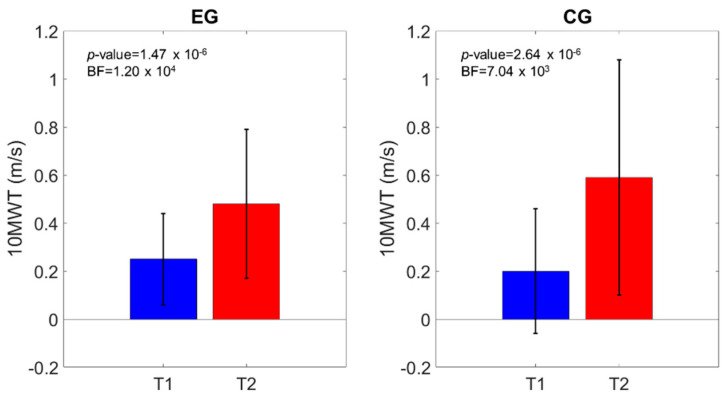
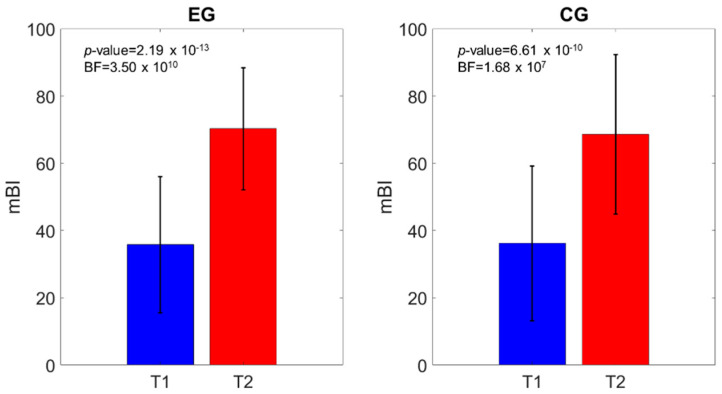
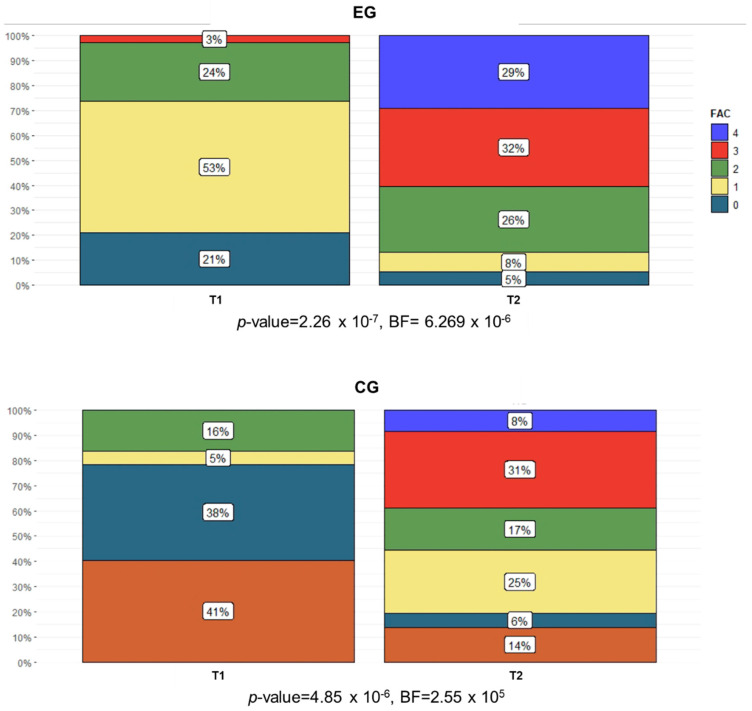
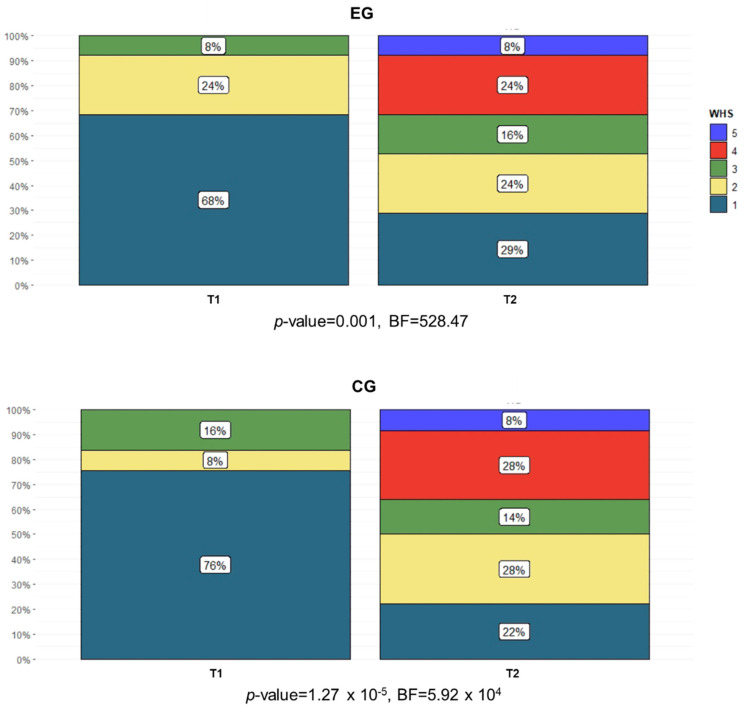
Results: The 6MWT increased in both groups, which was confirmed by both frequentist and Bayesian analyses. Similar outcomes were registered in the MI-AL, 10MWT, mBI, and MAS-AL. The FAC and WHS showed a significant number of subjects improving in functional and community ambulation in both groups at T2.
Conclusions: The clinical effects of o-RAGT were similar to conventional gait training in subacute stroke subjects. The results obtained in this study are encouraging and suggest future clinical trials on the topic.
Keywords: exoskeleton device; neurologic gait disorders; rehabilitation; robot-assisted gait training; stroke.
Conflict of interest statement
The authors certify that there is no conflict of interest with any financial organization or with the Ekso Bionics regarding the material discussed in the manuscript.
Figures
Similar articles
-
Overground wearable powered exoskeleton for gait training in subacute stroke subjects: clinical and gait assessments.Eur J Phys Rehabil Med. 2019 Dec;55(6):710-721. doi: 10.23736/S1973-9087.19.05574-6. Epub 2019 Feb 4. Eur J Phys Rehabil Med. 2019. PMID: 30723189
-
Functional Gait Recovery after a Combination of Conventional Therapy and Overground Robot-Assisted Gait Training Is Not Associated with Significant Changes in Muscle Activation Pattern: An EMG Preliminary Study on Subjects Subacute Post Stroke.Brain Sci. 2021 Apr 1;11(4):448. doi: 10.3390/brainsci11040448. Brain Sci. 2021. PMID: 33915808 Free PMC article.
-
Clinical efficacy of overground powered exoskeleton for gait training in patients with subacute stroke: A randomized controlled pilot trial.Medicine (Baltimore). 2023 Jan 27;102(4):e32761. doi: 10.1097/MD.0000000000032761. Medicine (Baltimore). 2023. PMID: 36705351 Free PMC article. Clinical Trial.
-
Efficacy of robotic exoskeleton for gait rehabilitation in patients with subacute stroke : a systematic review.Eur J Phys Rehabil Med. 2022 Feb;58(1):1-8. doi: 10.23736/S1973-9087.21.06846-5. Epub 2021 Jul 12. Eur J Phys Rehabil Med. 2022. PMID: 34247470 Free PMC article.
-
Efficacy of combined non-invasive brain stimulation and robot-assisted gait training on lower extremity recovery post-stroke: a systematic review and meta-analysis of randomized controlled trials.Front Neurol. 2025 Mar 7;16:1500020. doi: 10.3389/fneur.2025.1500020. eCollection 2025. Front Neurol. 2025. PMID: 40125401 Free PMC article.
Cited by
-
Hybrid robot-assisted gait training for motor function in subacute stroke: a single-blind randomized controlled trial.J Neuroeng Rehabil. 2022 Sep 14;19(1):99. doi: 10.1186/s12984-022-01076-6. J Neuroeng Rehabil. 2022. PMID: 36104706 Free PMC article. Clinical Trial.
-
A framework for clinical utilization of robotic exoskeletons in rehabilitation.J Neuroeng Rehabil. 2022 Oct 29;19(1):115. doi: 10.1186/s12984-022-01083-7. J Neuroeng Rehabil. 2022. PMID: 36309686 Free PMC article.
-
Exoskeletal wearable robot on ambulatory function in patients with stroke: a protocol for an international, multicentre, randomised controlled study.BMJ Open. 2023 Aug 11;13(8):e065298. doi: 10.1136/bmjopen-2022-065298. BMJ Open. 2023. PMID: 37567748 Free PMC article.
-
Longitudinal Changes in Temporospatial Gait Characteristics during the First Year Post-Stroke.Brain Sci. 2021 Dec 15;11(12):1648. doi: 10.3390/brainsci11121648. Brain Sci. 2021. PMID: 34942950 Free PMC article.
-
Interim results of exoskeletal wearable robot for gait recovery in subacute stroke patients.Sci Rep. 2025 Apr 5;15(1):11671. doi: 10.1038/s41598-025-96084-6. Sci Rep. 2025. PMID: 40188310 Free PMC article. Clinical Trial.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
