

Early Detection of Septic Shock Onset Using Interpretable Machine Learners
- PMID: 33467539
- PMCID: PMC7830968
- DOI: 10.3390/jcm10020301
Early Detection of Septic Shock Onset Using Interpretable Machine Learners
Abstract
Background: Developing a decision support system based on advances in machine learning is one area for strategic innovation in healthcare. Predicting a patient's progression to septic shock is an active field of translational research. The goal of this study was to develop a working model of a clinical decision support system for predicting septic shock in an acute care setting for up to 6 h from the time of admission in an integrated healthcare setting.
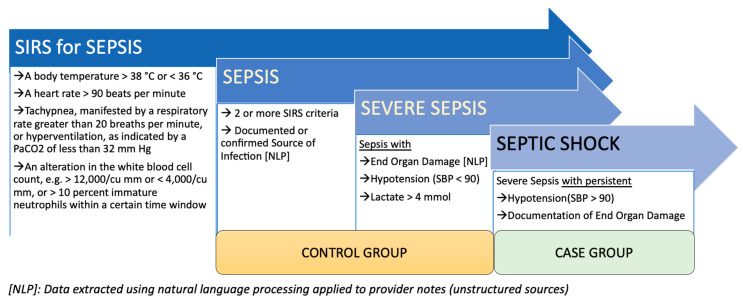
Method: Clinical data from Electronic Health Record (EHR), at encounter level, were used to build a predictive model for progression from sepsis to septic shock up to 6 h from the time of admission; that is, T = 1, 3, and 6 h from admission. Eight different machine learning algorithms (Random Forest, XGBoost, C5.0, Decision Trees, Boosted Logistic Regression, Support Vector Machine, Logistic Regression, Regularized Logistic, and Bayes Generalized Linear Model) were used for model development. Two adaptive sampling strategies were used to address the class imbalance. Data from two sources (clinical and billing codes) were used to define the case definition (septic shock) using the Centers for Medicare & Medicaid Services (CMS) Sepsis criteria. The model assessment was performed using Area under Receiving Operator Characteristics (AUROC), sensitivity, and specificity. Model predictions for each feature window (1, 3 and 6 h from admission) were consolidated.
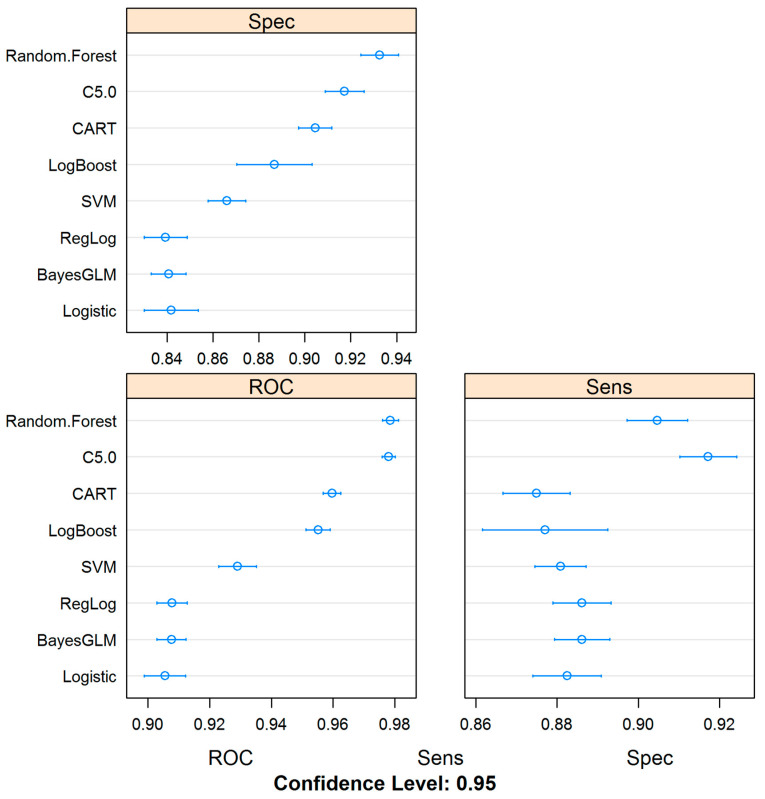
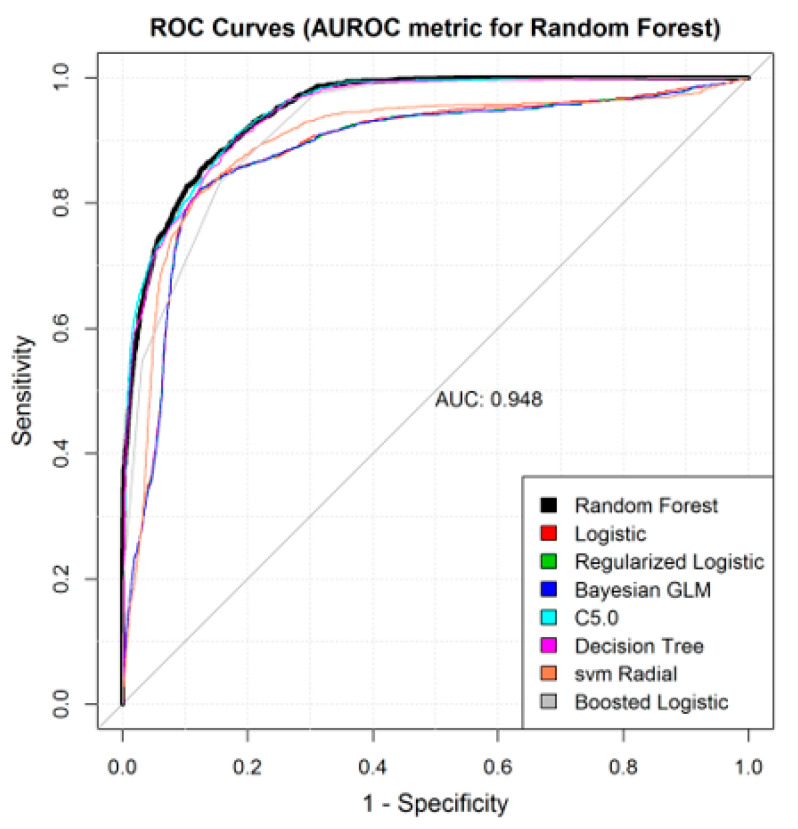
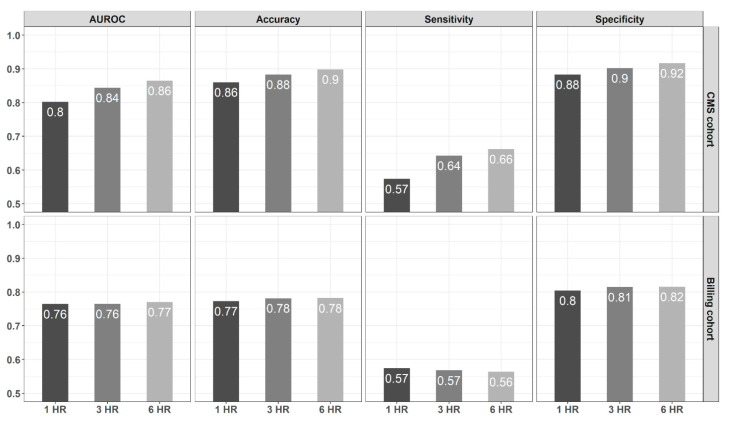
Results: Retrospective data from April 2005 to September 2018 were extracted from the EHR, Insurance Claims, Billing, and Laboratory Systems to create a dataset for septic shock detection. The clinical criteria and billing information were used to label patients into two classes-septic shock patients and sepsis patients at three different time points from admission, creating two different case-control cohorts. Data from 45,425 unique in-patient visits were used to build 96 prediction models comparing clinical-based definition versus billing-based information as the gold standard. Of the 24 consolidated models (based on eight machine learning algorithms and three feature windows), four models reached an AUROC greater than 0.9. Overall, all the consolidated models reached an AUROC of at least 0.8820 or higher. Based on the AUROC of 0.9483, the best model was based on Random Forest, with a sensitivity of 83.9% and specificity of 88.1%. The sepsis detection window at 6 h outperformed the 1 and 3-h windows. The sepsis definition based on clinical variables had improved performance when compared to the sepsis definition based on only billing information.
Conclusion: This study corroborated that machine learning models can be developed to predict septic shock using clinical and administrative data. However, the use of clinical information to define septic shock outperformed models developed based on only administrative data. Intelligent decision support tools can be developed and integrated into the EHR and improve clinical outcomes and facilitate the optimization of resources in real-time.
Keywords: artificial intelligence; clinical decision support system; electronic health record; explainable machine learning; healthcare; interpretable machine learning; machine learning; septic shock.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Kumar A., Roberts D., Wood K.E., Light B., Parrillo J.E., Sharma S., Suppes R., Feinstein D., Zanotti S., Taiberg L., et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock*. Crit. Care Med. 2006;34:1589–1596. doi: 10.1097/01.CCM.0000217961.75225.E9. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
