

Adenomyotic cyst mimicking a congenital Müllerian anomaly: Diagnosis and treatment with laparoscopy
- PMID: 33467841
- PMCID: PMC7943350
- DOI: 10.5653/cerm.2020.03867
Adenomyotic cyst mimicking a congenital Müllerian anomaly: Diagnosis and treatment with laparoscopy
Abstract
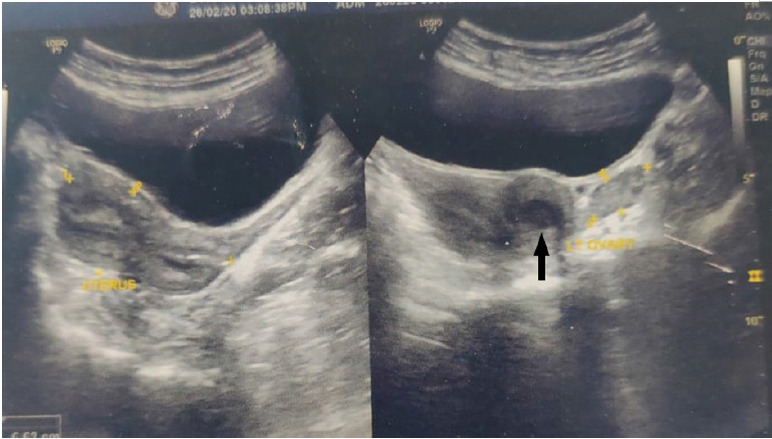
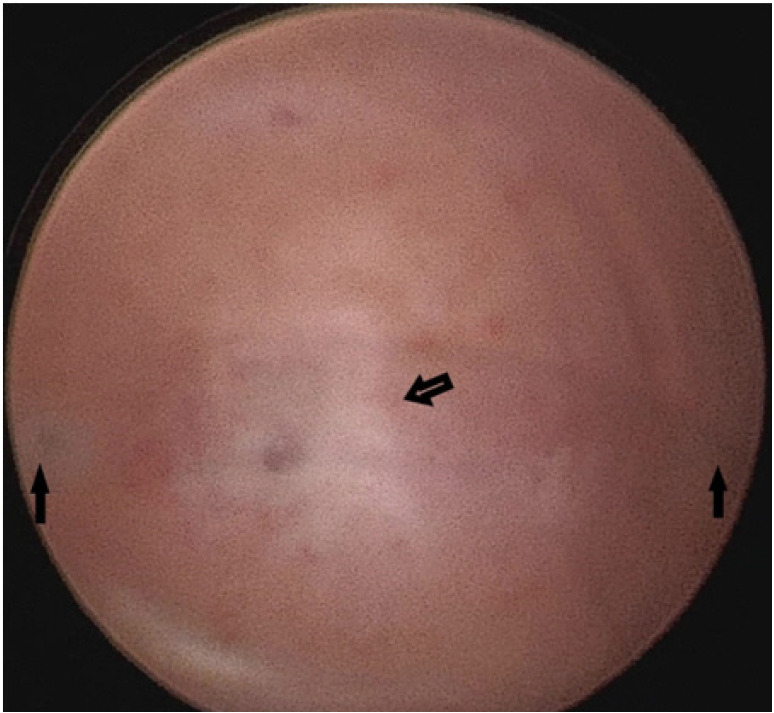
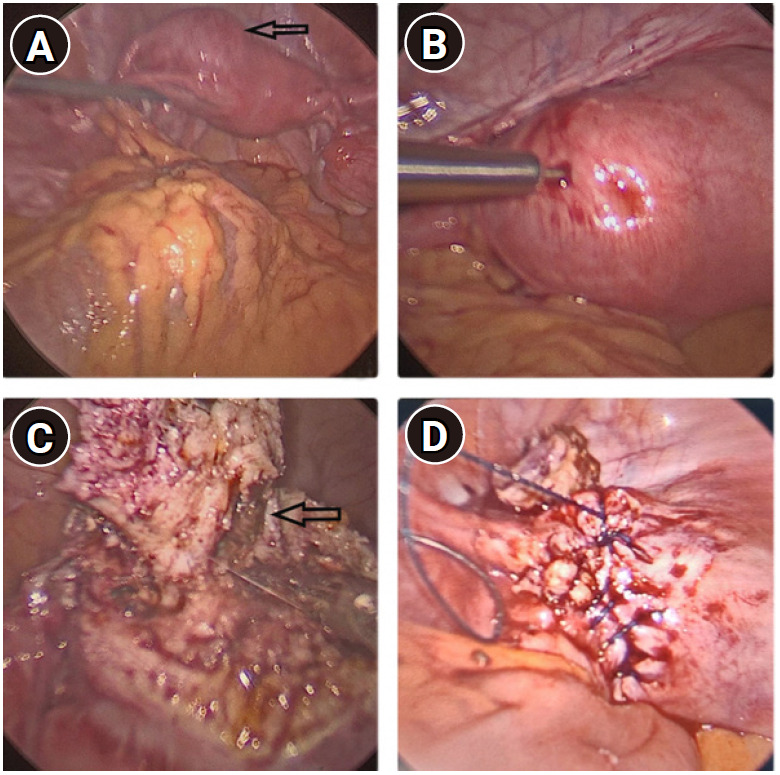
A 28-year-old woman presented with a 1-year history of severe progressive dysmenorrhea following suction evacuation and tubal ligation. Sonography showed a bicornuate uterus with hematometra in the left horn. Hysteroscopy ruled out a diagnosis of a congenital Müllerian anomaly, as both ostia appeared normal. Under laparoscopy, a mass was seen on the left fundal region near the insertion of the round ligament, and needle aspiration of a chocolate-colored fluid confirmed the diagnosis of an adenomyotic cyst. The cyst was excised. The patient recovered well and has been symptom-free since surgery. Adenomyotic cyst is a rare entity in young women and must be differentiated from obstructive Müllerian anomaly. Laparoscopy is the preferred minimally invasive modality for managing this rare disorder.
Keywords: Adenomyotic cyst; Dysmenorrhea; Laparoscopy; Obstructive Müllerian anomaly.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
An Exceptional Case of Complete Septate Uterus With Unilateral Cervical Aplasia (Class U2bC3V0/ESHRE/ESGE Classification) and Isolated Mullerian Remnants: Combined Hysteroscopic and Laparoscopic Treatment.J Minim Invasive Gynecol. 2016 Jan;23(1):16-7. doi: 10.1016/j.jmig.2015.09.006. Epub 2015 Sep 21. J Minim Invasive Gynecol. 2016. PMID: 26391060
-
Role of 3D Coronal Ultrasound in Diagnosis of Accessory and Cavitated Uterine Mass: A rare Mullerian Anomaly.J Obstet Gynaecol India. 2021 Dec;71(6):633-636. doi: 10.1007/s13224-021-01474-1. Epub 2021 May 2. J Obstet Gynaecol India. 2021. PMID: 34898903 Free PMC article.
-
Decidualized juvenile cystic adenomyoma mimicking a cornual pregnancy.Fertil Steril. 2020 Feb;113(2):463-465. doi: 10.1016/j.fertnstert.2019.10.026. Fertil Steril. 2020. PMID: 32106998
-
Diagnosis and treatment of müllerian malformations.Taiwan J Obstet Gynecol. 2020 Mar;59(2):183-188. doi: 10.1016/j.tjog.2020.01.003. Taiwan J Obstet Gynecol. 2020. PMID: 32127135 Review.
-
[The echographic diagnosis of a rare congenital uterine anomaly (uterus unicornis with a rudimentary noncommunicating horn)].Akush Ginekol (Sofiia). 1997;36(2):44-7. Akush Ginekol (Sofiia). 1997. PMID: 9471906 Review. Bulgarian.
Cited by
-
A case of large uterine cystic adenomyosis outside the uterus after laparoscopic myomectomy: a case report and literature review.BMC Womens Health. 2025 Jan 7;25(1):8. doi: 10.1186/s12905-024-03543-9. BMC Womens Health. 2025. PMID: 39762785 Free PMC article. Review.
-
Ultrasound-Guided Transvaginal Aspiration and Sclerotherapy for Uterine Cystic Adenomyosis: Case Report and Literature Review.Front Med (Lausanne). 2022 Mar 3;9:764523. doi: 10.3389/fmed.2022.764523. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35308513 Free PMC article.
References
-
- Cullen TS. Adenomyoma of the uterus. Philadelphia: Saunders; 1908.
-
- Parulekar SV. Cystic degeneration in an adenomyoma (a case report) J Postgrad Med. 1990;36:46–7. - PubMed
-
- Grimbizis GF, Mikos T, Tarlatzis B. Uterus-sparing operative treatment for adenomyosis. Fertil Steril. 2014;101:472–87. - PubMed
-
- Brosens I, Gordts S, Habiba M, Benagiano G. Uterine cystic adenomyosis: a disease of younger women. J Pediatr Adolesc Gynecol. 2015;28:420–6. - PubMed
-
- Takeda A, Sakai K, Mitsui T, Nakamura H. Laparoscopic management of juvenile cystic adenomyoma of the uterus: report of two cases and review of the literature. J Minim Invasive Gynecol. 2007;14:370–4. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
