

Diffusion-Weighted Imaging Lesions After Intracerebral Hemorrhage and Risk of Stroke: A MISTIE III and ATACH-2 Analysis
- PMID: 33467877
- PMCID: PMC8340082
- DOI: 10.1161/STROKEAHA.120.031628
Diffusion-Weighted Imaging Lesions After Intracerebral Hemorrhage and Risk of Stroke: A MISTIE III and ATACH-2 Analysis
Abstract
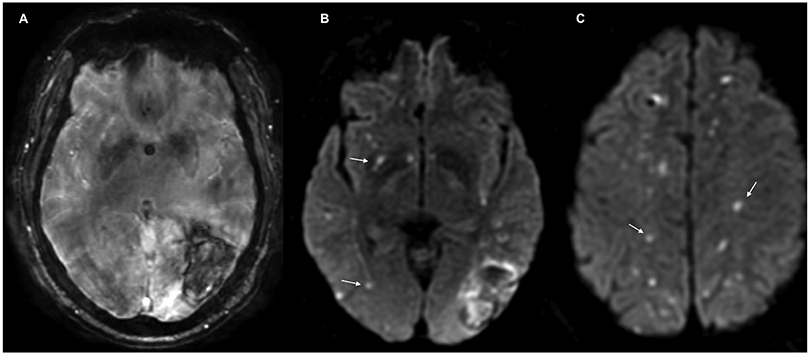
Background and purpose: Punctate ischemic lesions noted on diffusion-weighted imaging (DWI) are associated with poor functional outcomes after intracerebral hemorrhage (ICH). Whether these lesions increase long-term risk of stroke is poorly understood.
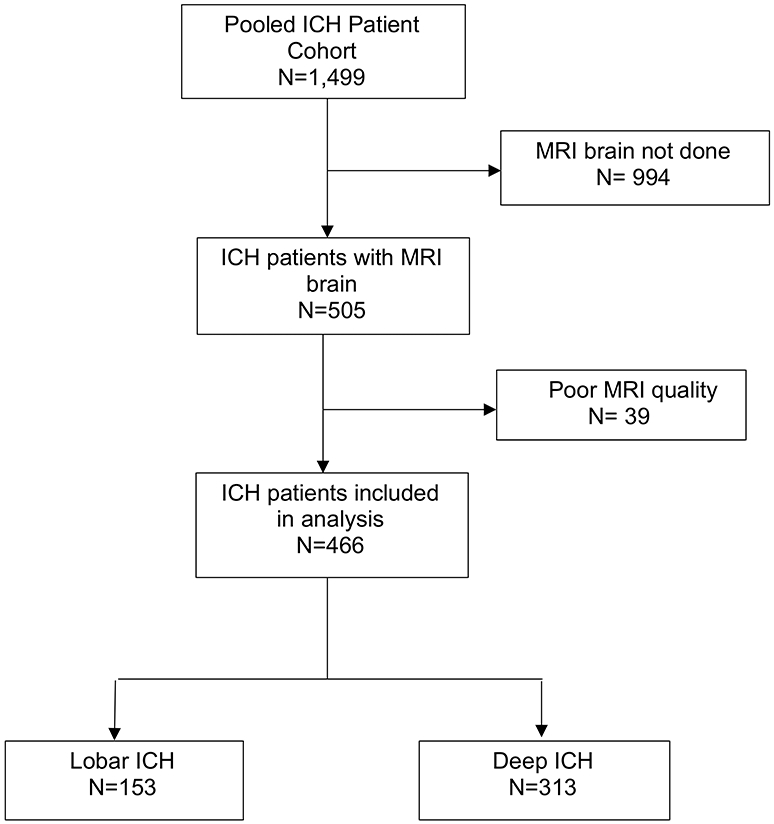
Methods: We pooled individual patient data from the ATACH-2 trial (Antihypertensive Treatment of Acute Cerebral Hemorrhage) and the MISTIE III trial (Minimally Invasive Surgery Plus Alteplase for Intracerebral Hemorrhage Evacuation Phase 3). We included subjects with a magnetic resonance imaging scan. The exposure was a DWI lesion. The primary outcome was any stroke, defined as a composite of ischemic stroke or recurrent ICH, whereas secondary outcomes were incident ischemic stroke and recurrent ICH. Using multivariate Cox regression analysis, we evaluated the risk of stroke.
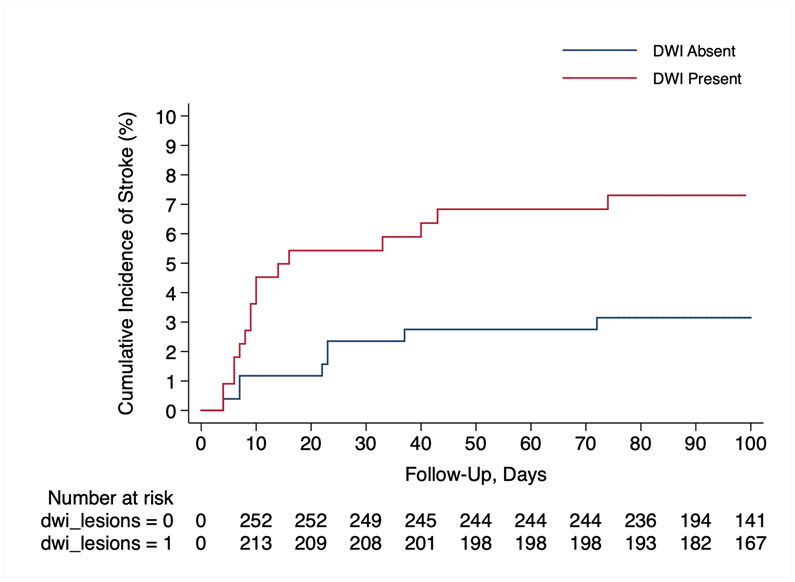
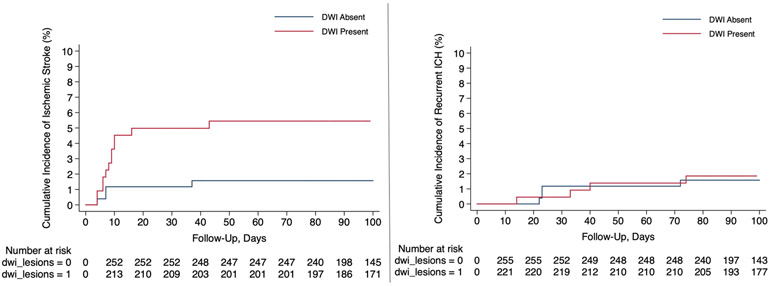
Results: Of 505 patients with ICH with magnetic resonance imaging, 466 were included. DWI lesions were noted in 214 (45.9%) subjects, and 34 incident strokes (20 ischemic stroke and 14 recurrent ICH) were observed during a median follow-up of 324 days (interquartile range, 91-374). Presence of a DWI lesion was associated with a 6.9% (95% CI, 2.2-11.6) absolute increase in risk of all stroke (hazard ratio, 2.6 [95% CI, 1.2-5.7]). Covariate adjustment with Cox regression models also demonstrated this increased risk. In the secondary analyses, there was an increased risk of ischemic stroke (hazard ratio, 3.5 [95% CI, 1.1-11.0]) but not recurrent ICH (hazard ratio, 1.7 [95% CI, 0.6-5.1]).
Conclusions: In a heterogeneous cohort of patients with ICH, presence of a DWI lesion was associated with a 2.5-fold heightened risk of stroke among ICH survivors. This elevated risk persisted for ischemic stroke but not for recurrent ICH.
Keywords: cerebral hemorrhage; hematoma; hypertension; magnetic resonance imaging; risk.
Figures
References
-
- Liotta EM, Singh M, Kosteva AR, Beaumont JL, Guth JC, Bauer RM, Prabhakaran S, Rosenberg NF, Maas MB, Naidech AM. Predictors of 30-Day Readmission after Intracerebral Hemorrhage: A Single-Center Approach for Identifying Potentially Modifiable Associations with Readmission. Crit Care Med. 2013;2762–2769 - PMC - PubMed
-
- Casolla B, Moulin S, Kyheng M, Henon H, Labreuche J, Leys D, Bauters C, Cordonnier C. Five-Year Risk of Major Ischemic and Hemorrhagic Events after Intracerebral Hemorrhage. Stroke. 2019;1100–1107 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 NR018335/NR/NINR NIH HHS/United States
- U24 NS107136/NS/NINDS NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- K76 AG059992/AG/NIA NIH HHS/United States
- P30 AG021342/AG/NIA NIH HHS/United States
- U24 TR001609/TR/NCATS NIH HHS/United States
- R03 NS112859/NS/NINDS NIH HHS/United States
- U24 NS107215/NS/NINDS NIH HHS/United States
- R01 NS073344/NS/NINDS NIH HHS/United States
- R01 NS102583/NS/NINDS NIH HHS/United States
- U01 NS080824/NS/NINDS NIH HHS/United States
- U01 NS062091/NS/NINDS NIH HHS/United States
- U01 NS095869/NS/NINDS NIH HHS/United States
- U01 NS106513/NS/NINDS NIH HHS/United States
- K23 NS105948/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
