

Long-term efficacy and safety of monotherapy with a single fresh fecal microbiota transplant for recurrent active ulcerative colitis: a prospective randomized pilot study
- PMID: 33468164
- PMCID: PMC7816432
- DOI: 10.1186/s12934-021-01513-6
Long-term efficacy and safety of monotherapy with a single fresh fecal microbiota transplant for recurrent active ulcerative colitis: a prospective randomized pilot study
Abstract
Background: To assess the long-term safety and efficacy of monotherapy with a single fresh fecal microbiota transplant (FMT) for recurrent ulcerative colitis (UC).
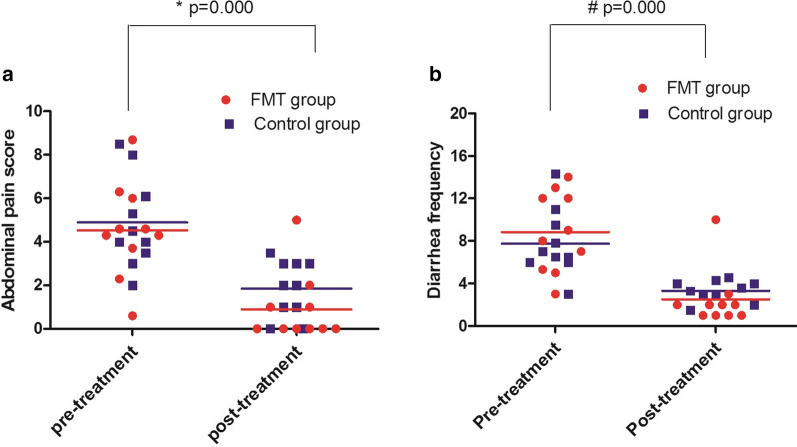
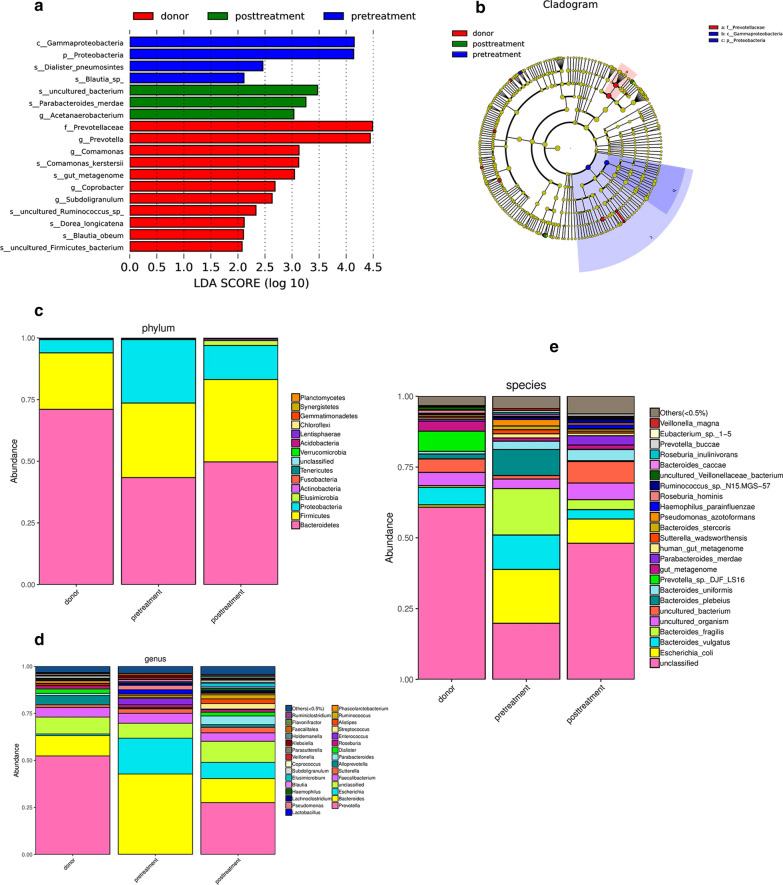
Results: Twenty-six eligible patients were enrolled, and 6 patients were excluded. Ultimately, 20 patients were randomized to the FMT group (n = 10) and the control group (n = 10); 80% were females (F/M = 16/4), the mean age was 48 ± 14 years, and the mean duration was 6.4 ± 8.2 years. The mean length of post-FMT follow-up was 19.1 ± 10.1 months (6-38). No statistically significant differences in baseline demographic or clinical characteristics were found between the groups. Ninety percent of patients in the FMT group and 50% of patients in the control group met the primary endpoint at week 8. The Mayo score was significantly decreased compared with that of the control group (n = 10) when reassessed at week 4 (P = 0.001) and week 8 (P = 0.019) after FMT; there was no significant difference 6 months after treatment. The median remission time was 24 months (95% CI 68.26-131.7%) in both the FMT (range 6-38 months) and control groups (range 7-35 months), with no significant difference (P = 0.895). Participants tolerated FMT treatment, and no adverse events occurred during long-term follow-up, with one treatment-related significant adverse event (EBV infection) occurring within 2 weeks after FMT. Stool microbiota composition analysis indicated improved gut microbiota diversity after FMT, with expansion of stool-donor taxa. Bacteroidetes, Firmicutes and Proteobacteria were the dominant bacterial phyla of the gut microbiota in active UC patients. The relative abundance of Bacteroidetes decreased and that of Proteobacteria increased significantly in active UC patients compared with donors, while Firmicutes showed no significant changes. A single fresh FMT could effectively reconstruct the gut microbiota composition in patients with active UC and maintain stability, with increased Bacteroidetes and decreased Proteobacteria abundance. FMT significantly reduced the relative abundance of Escherichia and increased the relative abundance of Prevotella at the genus level. Pyruvate metabolism, glyoxylate and dicarboxylate metabolism, and pantothenate and CoA biosynthesis showed significant differences after transplantation.
Conclusions: Monotherapy with a single fresh FMT is an effective and safe strategy to induce long-term remission without drugs in patients with active UC and may be an alternative induction therapy for recurrent UC or even primary UC.
Keywords: Fecal microbiota transplantation; Gut microbiota; Inflammatory bowel disease; Intestinal flora; Ulcerative colitis.
Conflict of interest statement
The authors have no financial or potential competing interests or affiliations with any institution, organization, or company relating to the manuscript.
Figures


Similar articles
-
Longitudinal microbiome analysis of single donor fecal microbiota transplantation in patients with recurrent Clostridium difficile infection and/or ulcerative colitis.PLoS One. 2018 Jan 31;13(1):e0190997. doi: 10.1371/journal.pone.0190997. eCollection 2018. PLoS One. 2018. PMID: 29385143 Free PMC article.
-
Fecal Microbiota Transplantation for Ulcerative Colitis: The Optimum Timing and Gut Microbiota as Predictors for Long-Term Clinical Outcomes.Clin Transl Gastroenterol. 2020 Aug;11(8):e00224. doi: 10.14309/ctg.0000000000000224. Clin Transl Gastroenterol. 2020. PMID: 32955197 Free PMC article.
-
Efficacy and safety of single fecal microbiota transplantation for Japanese patients with mild to moderately active ulcerative colitis.J Gastroenterol. 2017 Apr;52(4):476-482. doi: 10.1007/s00535-016-1271-4. Epub 2016 Oct 11. J Gastroenterol. 2017. PMID: 27730312 Clinical Trial.
-
Fecal transplantation for treatment of inflammatory bowel disease.Cochrane Database Syst Rev. 2018 Nov 13;11(11):CD012774. doi: 10.1002/14651858.CD012774.pub2. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2023 Apr 25;4:CD012774. doi: 10.1002/14651858.CD012774.pub3. PMID: 30480772 Free PMC article. Updated.
-
Fecal microbiota transplantation for ulcerative colitis.Immunol Med. 2021 Mar;44(1):30-34. doi: 10.1080/25785826.2020.1792040. Epub 2020 Jul 14. Immunol Med. 2021. PMID: 32663072 Review.
Cited by
-
Cross-Talk Between Butyric Acid and Gut Microbiota in Ulcerative Colitis Following Fecal Microbiota Transplantation.Front Microbiol. 2021 Apr 12;12:658292. doi: 10.3389/fmicb.2021.658292. eCollection 2021. Front Microbiol. 2021. PMID: 33912150 Free PMC article.
-
An Immunologic Compatibility Testing Was Not Useful for Donor Selection in Fecal Microbiota Transplantation for Ulcerative Colitis.Front Immunol. 2021 Jun 4;12:683387. doi: 10.3389/fimmu.2021.683387. eCollection 2021. Front Immunol. 2021. PMID: 34149723 Free PMC article.
-
Association between Intestinal Microecological Changes and Atherothrombosis.Microorganisms. 2023 May 6;11(5):1223. doi: 10.3390/microorganisms11051223. Microorganisms. 2023. PMID: 37317197 Free PMC article. Review.
-
Role of gut microbiota and mesenteric adipose tissue in the pathology of Crohn's disease: Potential therapeutic targets.World J Gastroenterol. 2025 Apr 7;31(13):102291. doi: 10.3748/wjg.v31.i13.102291. World J Gastroenterol. 2025. PMID: 40248060 Free PMC article.
-
Safety and efficacy of fecal microbiota transplantation for viral diseases: A systematic review of clinical trials.PLoS One. 2024 Oct 21;19(10):e0311731. doi: 10.1371/journal.pone.0311731. eCollection 2024. PLoS One. 2024. PMID: 39432486 Free PMC article.
References
-
- Ng SC, Shi HY, Hamidi N, Underwood FE, Tang W, Benchimol EI, Panaccione R, Ghosh S, Wu JCY, Chan FKL, Sung JJY, Kaplan GG. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2018;390(10114):2769–2778. doi: 10.1016/S0140-6736(17)32448-0. - DOI - PubMed
-
- Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, ChernoffG, Benchimol EI, Panaccione R, Ghosh S, Barkema HW, Kaplan GG. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology 2012;142(1):46–54.e42 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
