

Avoiding a Med-Wreck: a structured medication reconciliation framework and standardized auditing tool utilized to optimize patient safety and reallocate hospital resources
- PMID: 33468248
- PMCID: PMC7814270
- DOI: 10.1186/s40545-021-00296-w
Avoiding a Med-Wreck: a structured medication reconciliation framework and standardized auditing tool utilized to optimize patient safety and reallocate hospital resources
Abstract
Background: The incidence of preventable adverse drug events (ADE) is approximately one medication error per patient per hospital-day. A quality medication reconciliation (MedRec) process is a crucial intervention used to reduce ADE in the hospital and community setting. Amid the coronavirus disease 2019 (COVID-19) pandemic, preventing medication errors is vital to avoid patient readmission, reduce disease complications, and reduce cost and patient burden on the healthcare system.
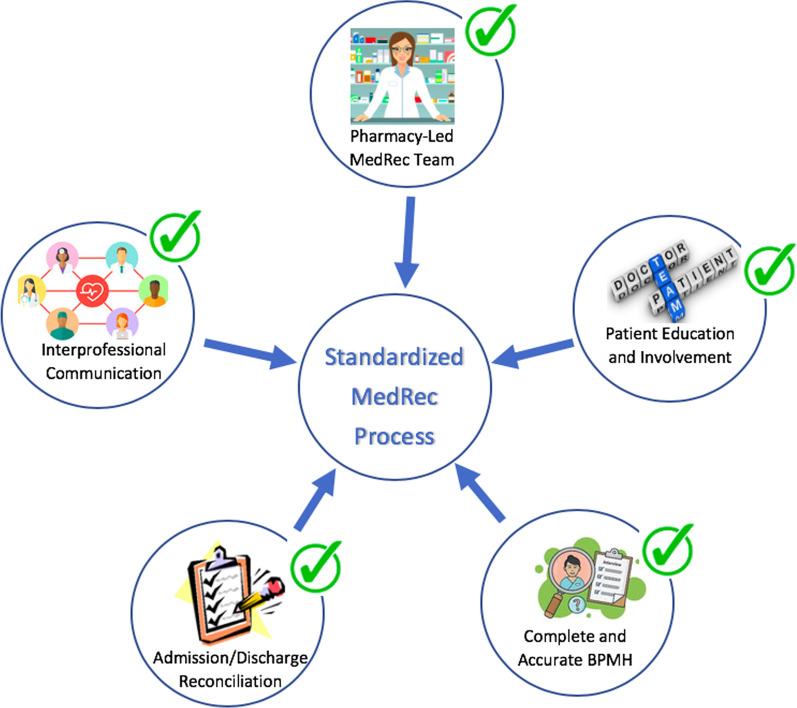
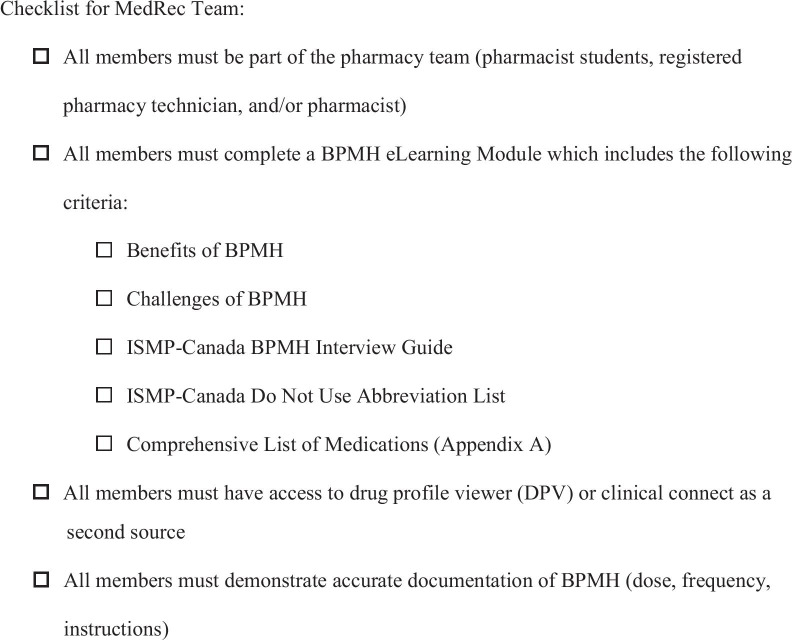
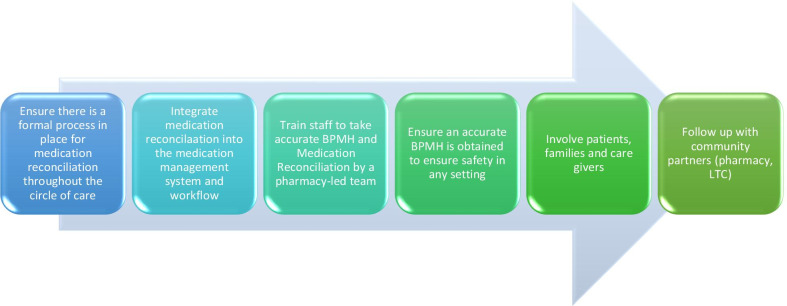
Objectives: To develop a standardized MedRec framework that can be implemented in all healthcare settings to reduce patient and staff harm during COVID-19. Also, to create a standardized auditing tool used to assess the quality of the MedRec process and allow for continuous quality improvement.
Methods: A multi-site gap analysis (MGA) was performed to collect observational data that were collected from four different healthcare sites (two hospitals, a long-term care facility, and a community pharmacy). MGA consists of collecting data across several sites which answer a standardized questionnaire. A standardized MedRec framework and auditing tool were developed based on the gaps observed in each site and literature reviews.
Results: A standardized MedRec process was not implemented in any of the observed sites. The healthcare sites lacked a designated MedRec team and training related to the MedRec process leading to multiple discrepancies at discharge. Patients were not counselled on changes to home medications, and a discharge report was often not provided upon discharge. Communication mechanisms between community pharmacies and hospital physicians are not available or easily accessible.
Conclusion: The proposed structured MedRec framework is vital to reduce medication errors and patient harm amid COVID-19. Moreover, the comprehensive auditing tool developed in this study allows for continuous quality improvement resulting in superior quality care, reduction of workflow inefficiencies, cost savings on hospital readmissions, and overall enhanced healthcare system performance.
Keywords: Auditing tool; COVID-19; Cost-effective analysis; Medication errors; Medication reconciliation.
Conflict of interest statement
No known competing interest to declare.
Figures
Similar articles
-
Differences in medication reconciliation interventions between six hospitals: a mixed method study.BMC Health Serv Res. 2022 May 31;22(1):722. doi: 10.1186/s12913-022-08118-8. BMC Health Serv Res. 2022. PMID: 35642033 Free PMC article.
-
Evaluation of a Novel Audit Tool for Medication Reconciliation at Hospital Discharge.Can J Hosp Pharm. 2019 Nov-Dec;72(6):421-427. Epub 2019 Dec 1. Can J Hosp Pharm. 2019. PMID: 31853142 Free PMC article.
-
Process mapping evaluation of medication reconciliation in academic teaching hospitals: a critical step in quality improvement.BMJ Open. 2016 Dec 30;6(12):e013663. doi: 10.1136/bmjopen-2016-013663. BMJ Open. 2016. PMID: 28039294 Free PMC article.
-
Exploring the contextual and human factors of electronic medication reconciliation research: a scoping review.Stud Health Technol Inform. 2013;194:166-72. Stud Health Technol Inform. 2013. PMID: 23941950
-
Use of information technology in medication reconciliation: a scoping review.Ann Pharmacother. 2010 May;44(5):885-97. doi: 10.1345/aph.1M699. Epub 2010 Apr 6. Ann Pharmacother. 2010. PMID: 20371752
Cited by
-
A national survey on assessment of knowledge, perceptions, practice, and barriers among hospital pharmacists towards medication reconciliation in United Arab Emirates.Sci Rep. 2024 Jul 4;14(1):15370. doi: 10.1038/s41598-024-64605-4. Sci Rep. 2024. PMID: 38965258 Free PMC article.
-
Revisiting acidosis in acetazolamide treatment of severe glaucoma: A case report.Am J Ophthalmol Case Rep. 2022 Jul 6;27:101658. doi: 10.1016/j.ajoc.2022.101658. eCollection 2022 Sep. Am J Ophthalmol Case Rep. 2022. PMID: 35845746 Free PMC article. No abstract available.
-
Effect of educational intervention on medication reconciliation practice of hospital pharmacists in a developing country - A non-randomised controlled trial.BMC Med Educ. 2023 Nov 15;23(1):867. doi: 10.1186/s12909-023-04844-7. BMC Med Educ. 2023. PMID: 37968602 Free PMC article. Clinical Trial.
-
Differences in medication reconciliation interventions between six hospitals: a mixed method study.BMC Health Serv Res. 2022 May 31;22(1):722. doi: 10.1186/s12913-022-08118-8. BMC Health Serv Res. 2022. PMID: 35642033 Free PMC article.
-
Optimisation of medication reconciliation using queueing theory: a computer experiment.Int J Clin Pharm. 2024 Aug;46(4):881-888. doi: 10.1007/s11096-024-01722-0. Epub 2024 May 10. Int J Clin Pharm. 2024. PMID: 38727777
References
-
- Preventing medication errors. Institute of Medicine; 2006.
-
- Terry A, Mottram C, Round J, Firman E, Step J, Bourne J. A safer place for patients: learning to improve patient safety. New York: National Audit Office; 2005.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous