

Effectiveness of very low profile thrombectomy device in primary distal medium vessel occlusion, as rescue therapy after incomplete proximal recanalization or following iatrogenic thromboembolic events
- PMID: 33468609
- PMCID: PMC8606433
- DOI: 10.1136/neurintsurg-2020-017035
Effectiveness of very low profile thrombectomy device in primary distal medium vessel occlusion, as rescue therapy after incomplete proximal recanalization or following iatrogenic thromboembolic events
Abstract
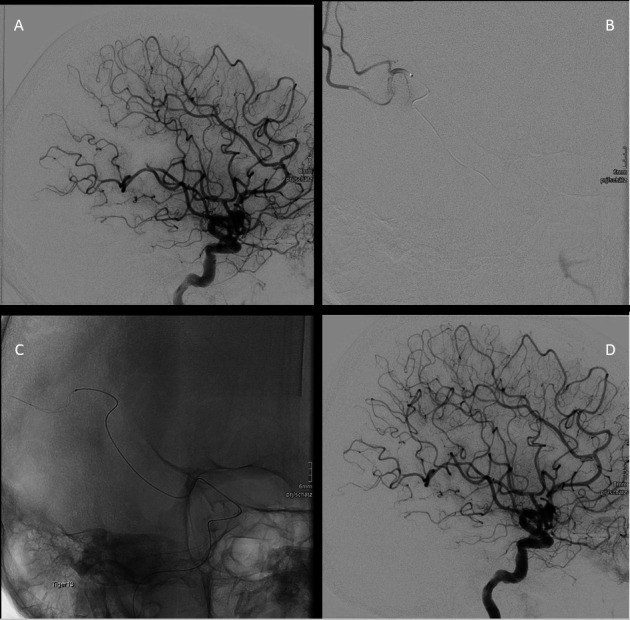
Background: Recent progress with smaller retrievers has expanded the ability to reach distal brain arteries. We herein report recanalization, bleeding complications and short-term clinical outcomes with the smallest currently known low profile thrombectomy device in patients with primary or secondary distal medium vessel occlusion (DMVO).
Methods: We performed a retrospective analysis of 115 patients receiving mechanical thrombectomy (MT) in DMVO using the extended Thrombolysis in Cerebral Infarction (eTICI), European Cooperative Acute Stroke Study (ECASS) II classification, The National Institutes of Health Stroke Scale (NIHSS) and modified Rankin Scale (mRS) scores at admission and discharge to evaluate outcomes. Patients were stratified into three groups: (1) primary isolated distal occlusion (n=34), (2) secondary distal occlusion after MT of a proximal vessel occlusion (n=71), or (3) during endovascular treatment of aneurysms or arteriovenous malformations (AVMs) (n=10).
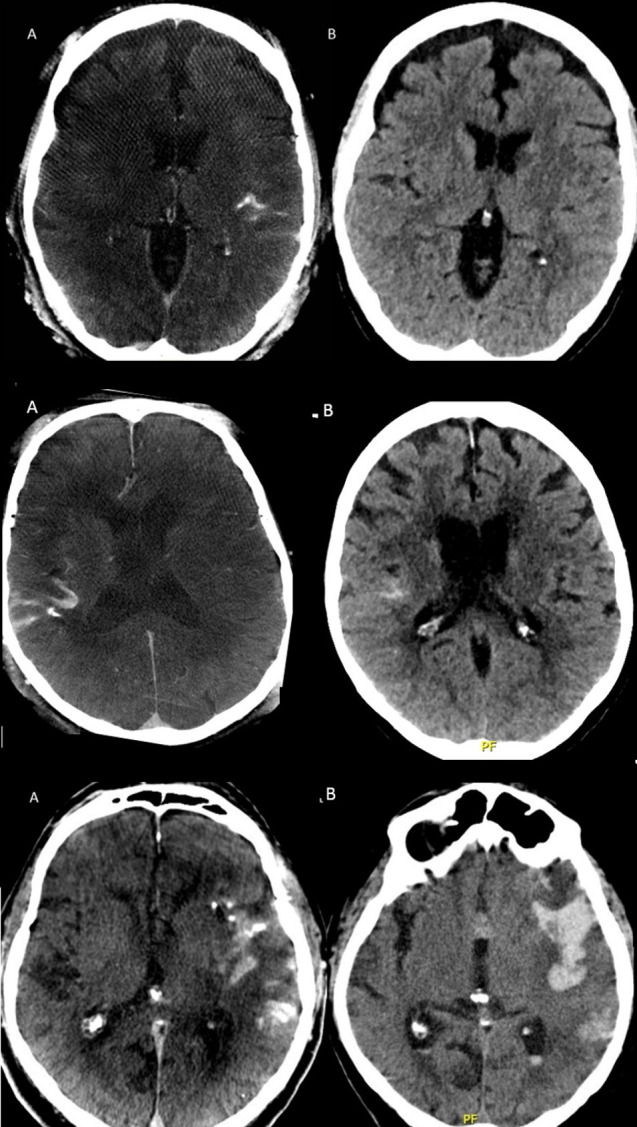
Results: Successful distal recanalization, defined as an eTICI score of 2b67, 2c and 3, was achieved in 74.7% (86/115) of patients. More specifically, it was 70.5% (24/34), 73.2% (52/71), and 100% (10/10) of primary DMVO, secondary DMVO after proximal MT, and rescue MT during aneurysm or AVM embolization, respectively. Symptomatic intraparenchymal bleeding occurred in 6.9% (eight patients). In-hospital mortality occurred in 18.1% (19/105) of patients with stroke. The most common cause of death was large infarct, old age, and therapy limitation.
Conclusion: Direct or rescue MT of DMVO using a very low profile thrombectomy device is associated with a high rate of successful recanalization and a reasonable rate of symptomatic hemorrhagic complication, despite a risk of 18.1% hospital mortality in elderly patients. Further trials are needed to confirm our results and assess long-term clinical outcomes.
Keywords: stent; stroke; thrombectomy; thrombolysis.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: RC received consulting fee or speaker honoraria from Balt, Medtronic, Microvention, Rapid Medical, Siemens and Stryker. PJM receives public funding related to intracranial aneurysm and vasospasm therapy from the Swiss National Science Foundation and the Innosuisse agency. RW received speaker honoria from Bristol Myers Squibb. RR received a travel grant from Boehringer Ingelheim and Microvention.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical