

SARS-CoV-2 Infection Severity Is Linked to Superior Humoral Immunity against the Spike
- PMID: 33468695
- PMCID: PMC7845638
- DOI: 10.1128/mBio.02940-20
SARS-CoV-2 Infection Severity Is Linked to Superior Humoral Immunity against the Spike
Abstract
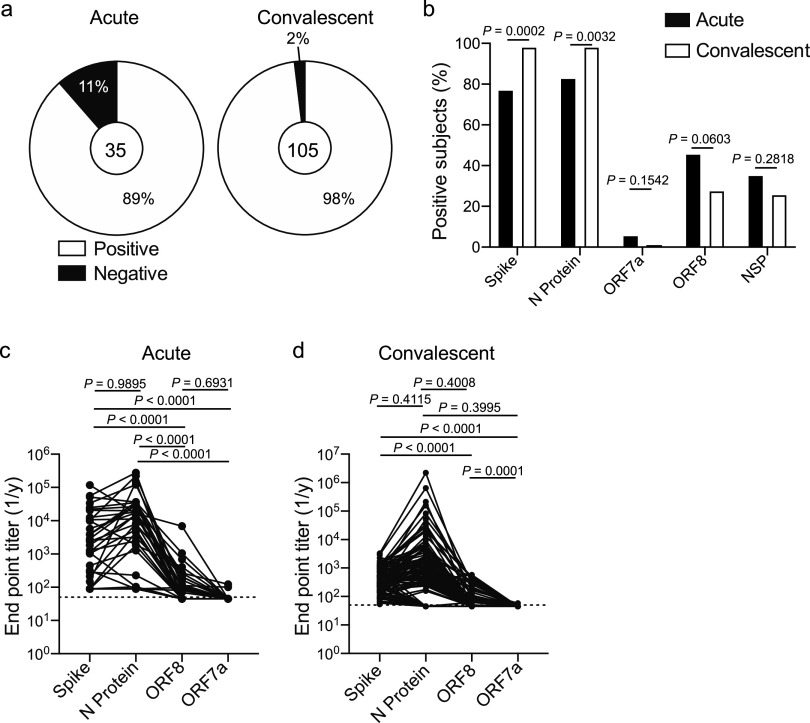
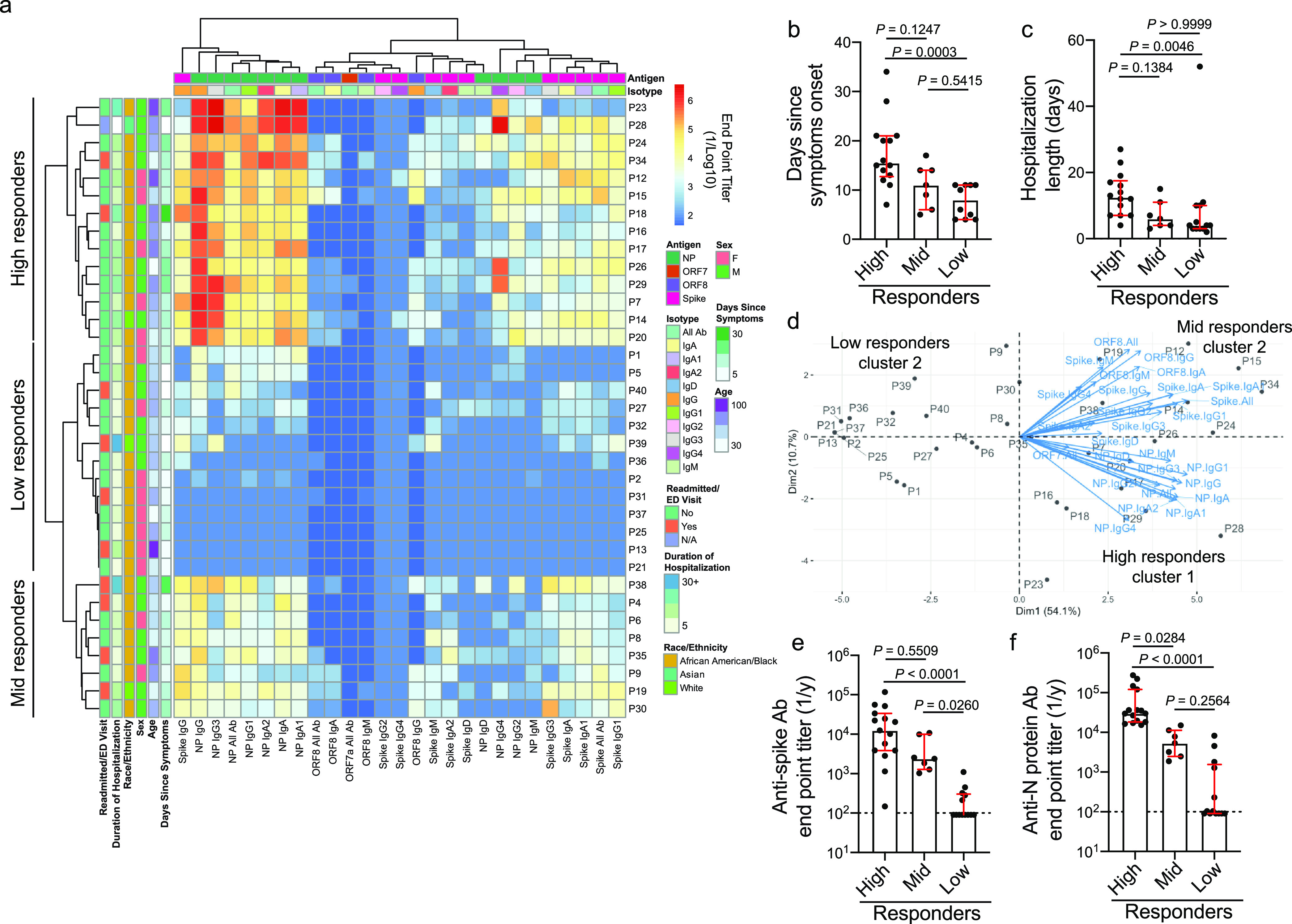
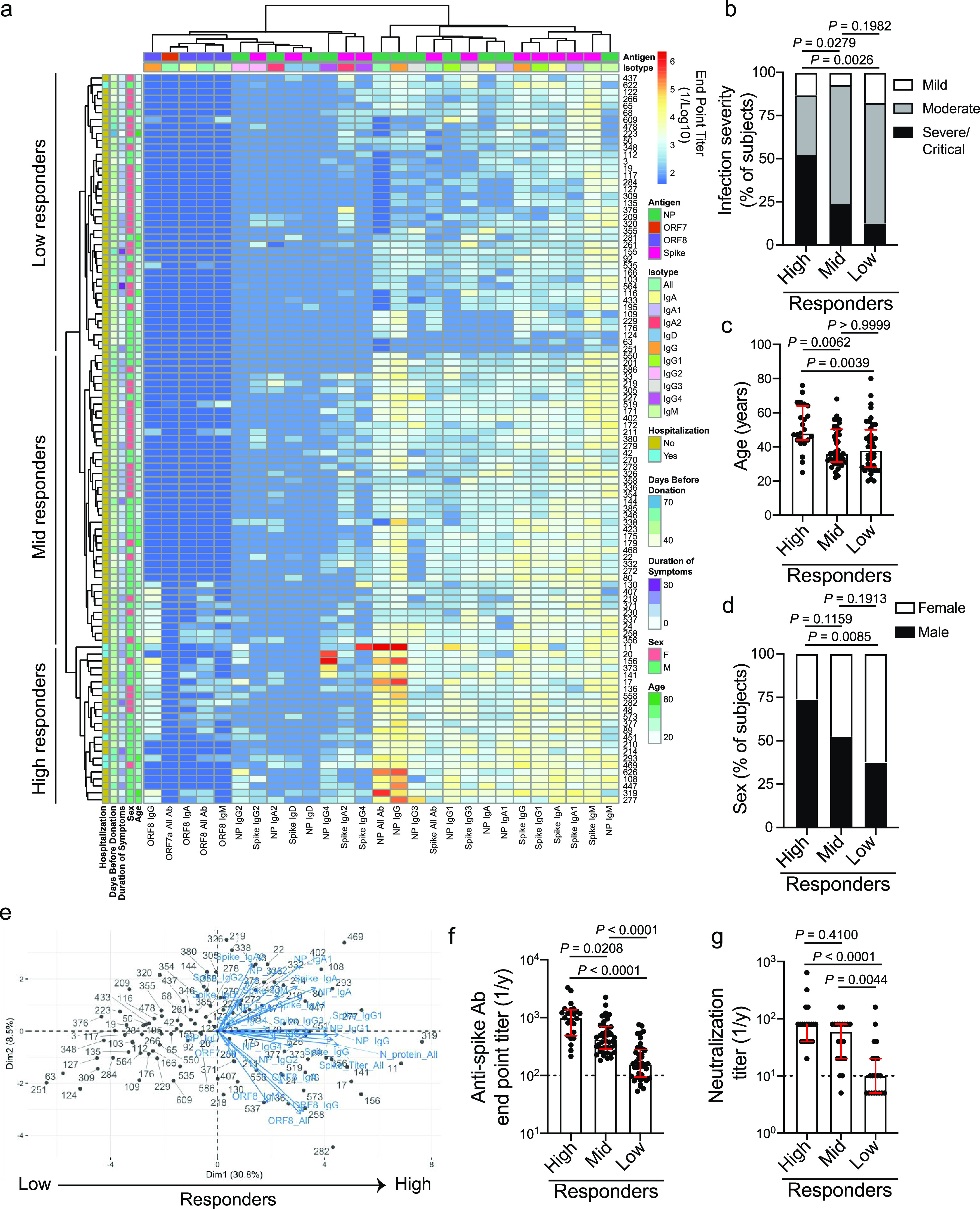
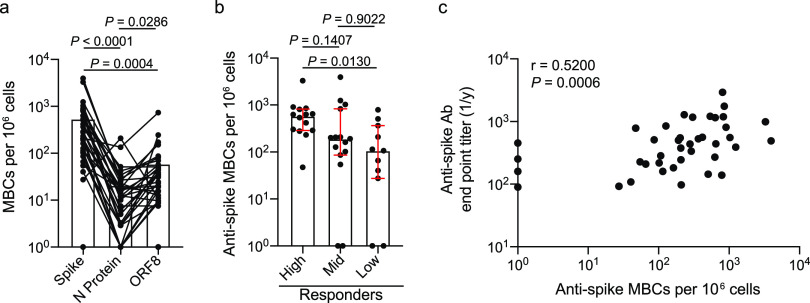
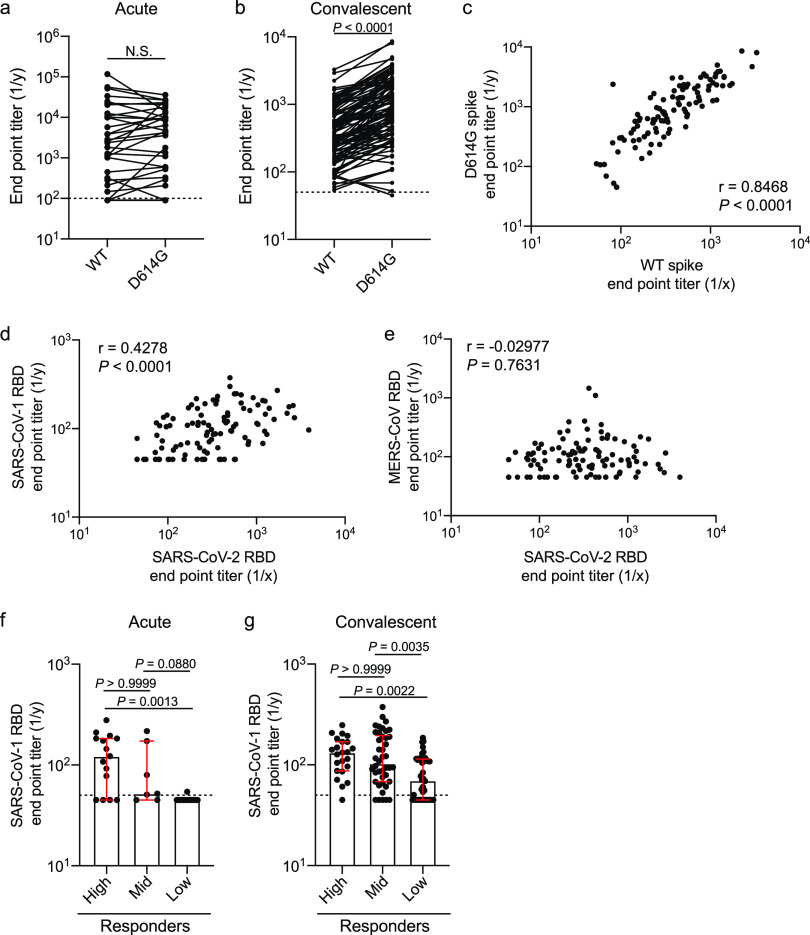
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is currently causing a global pandemic. The antigen specificity of the antibody response mounted against this novel virus is not understood in detail. Here, we report that subjects with a more severe SARS-CoV-2 infection exhibit a larger antibody response against the spike and nucleocapsid protein and epitope spreading to subdominant viral antigens, such as open reading frame 8 and nonstructural proteins. Subjects with a greater antibody response mounted a larger memory B cell response against the spike, but not the nucleocapsid protein. Additionally, we revealed that antibodies against the spike are still capable of binding the D614G spike mutant and cross-react with the SARS-CoV-1 receptor binding domain. Together, this study reveals that subjects with a more severe SARS-CoV-2 infection exhibit a greater overall antibody response to the spike and nucleocapsid protein and a larger memory B cell response against the spike.IMPORTANCE With the ongoing pandemic, it is critical to understand how natural immunity against SARS-CoV-2 and COVID-19 develops. We have identified that subjects with more severe COVID-19 disease mount a more robust and neutralizing antibody response against SARS-CoV-2 spike protein. Subjects who mounted a larger response against the spike also mounted antibody responses against other viral antigens, including the nucleocapsid protein and ORF8. Additionally, this study reveals that subjects with more severe disease mount a larger memory B cell response against the spike. These data suggest that subjects with more severe COVID-19 disease are likely better protected from reinfection with SARS-CoV-2.
Keywords: SARS-CoV-2; humoral immunity; infection severity; memory B cells; neutralizing antibodies.
Copyright © 2021 Guthmiller et al.
Figures
Update of
-
SARS-CoV-2 infection severity is linked to superior humoral immunity against the spike.bioRxiv [Preprint]. 2020 Sep 13:2020.09.12.294066. doi: 10.1101/2020.09.12.294066. bioRxiv. 2020. Update in: mBio. 2021 Jan 19;12(1):e02940-20. doi: 10.1128/mBio.02940-20. PMID: 32935099 Free PMC article. Updated. Preprint.
Similar articles
-
SARS-CoV-2 infection severity is linked to superior humoral immunity against the spike.bioRxiv [Preprint]. 2020 Sep 13:2020.09.12.294066. doi: 10.1101/2020.09.12.294066. bioRxiv. 2020. Update in: mBio. 2021 Jan 19;12(1):e02940-20. doi: 10.1128/mBio.02940-20. PMID: 32935099 Free PMC article. Updated. Preprint.
-
Mild SARS-CoV-2 Illness Is Not Associated with Reinfections and Provides Persistent Spike, Nucleocapsid, and Virus-Neutralizing Antibodies.Microbiol Spectr. 2021 Oct 31;9(2):e0008721. doi: 10.1128/Spectrum.00087-21. Epub 2021 Sep 1. Microbiol Spectr. 2021. PMID: 34468184 Free PMC article.
-
Deciphering the Role of Humoral and Cellular Immune Responses in Different COVID-19 Vaccines-A Comparison of Vaccine Candidate Genes in Roborovski Dwarf Hamsters.Viruses. 2021 Nov 16;13(11):2290. doi: 10.3390/v13112290. Viruses. 2021. PMID: 34835096 Free PMC article.
-
Characterization of SARS-CoV-2-specific humoral immunity and its potential applications and therapeutic prospects.Cell Mol Immunol. 2022 Feb;19(2):150-157. doi: 10.1038/s41423-021-00774-w. Epub 2021 Oct 13. Cell Mol Immunol. 2022. PMID: 34645940 Free PMC article. Review.
-
The Key to Increase Immunogenicity of Next-Generation COVID-19 Vaccines Lies in the Inclusion of the SARS-CoV-2 Nucleocapsid Protein.J Immunol Res. 2024 May 29;2024:9313267. doi: 10.1155/2024/9313267. eCollection 2024. J Immunol Res. 2024. PMID: 38939745 Free PMC article. Review.
Cited by
-
SARS-CoV-2 immunity in animal models.Cell Mol Immunol. 2024 Feb;21(2):119-133. doi: 10.1038/s41423-023-01122-w. Epub 2024 Jan 18. Cell Mol Immunol. 2024. PMID: 38238440 Free PMC article. Review.
-
Structure of a Vaccine-Induced, Germline-Encoded Human Antibody Defines a Neutralizing Epitope on the SARS-CoV-2 Spike N-Terminal Domain.mBio. 2022 Jun 28;13(3):e0358021. doi: 10.1128/mbio.03580-21. Epub 2022 Apr 25. mBio. 2022. PMID: 35467422 Free PMC article.
-
Airway antibodies emerge according to COVID-19 severity and wane rapidly but reappear after SARS-CoV-2 vaccination.JCI Insight. 2021 Nov 22;6(22):e151463. doi: 10.1172/jci.insight.151463. JCI Insight. 2021. PMID: 34665783 Free PMC article.
-
Passive Immunity Should and Will Work for COVID-19 for Some Patients.Clin Hematol Int. 2021 Apr 16;3(2):47-68. doi: 10.2991/chi.k.210328.001. eCollection 2021 Jun. Clin Hematol Int. 2021. PMID: 34595467 Free PMC article. Review.
-
Functional importance of the D614G mutation in the SARS-CoV-2 spike protein.Biochem Biophys Res Commun. 2021 Jan 29;538:108-115. doi: 10.1016/j.bbrc.2020.11.026. Epub 2020 Nov 13. Biochem Biophys Res Commun. 2021. PMID: 33220921 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
