

Clinical and laboratory features of hypercoagulability in COVID-19 and other respiratory viral infections amongst predominantly younger adults with few comorbidities
- PMID: 33469056
- PMCID: PMC7815883
- DOI: 10.1038/s41598-021-81166-y
Clinical and laboratory features of hypercoagulability in COVID-19 and other respiratory viral infections amongst predominantly younger adults with few comorbidities
Abstract
COVID-19 caused by Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) and other respiratory viral (non-CoV-2-RV) infections are associated with thrombotic complications. The differences in prothrombotic potential between SARS-CoV-2 and non-CoV-2-RV have not been well characterised. We compared the thrombotic rates between these two groups of patients directly and further delved into their coagulation profiles. In this single-center, retrospective cohort study, all consecutive COVID-19 and non-CoV-2-RV patients admitted between January 15th and April 10th 2020 were included. Coagulation parameters studied were prothrombin time and activated partial thromboplastin time and its associated clot waveform analysis (CWA) parameter, min1, min2 and max2. In the COVID-19 (n = 181) group there were two (1.0 event/1000-hospital-days) myocardial infarction events while one (1.8 event/1000-hospital-day) was reported in the non-CoV-2-RV (n = 165) group. These events occurred in patients who were severely ill. There were no venous thrombotic events. Coagulation parameters did not differ throughout the course of mild COVID-19. However, CWA parameters were significantly higher in severe COVID-19 compared with mild disease, suggesting hypercoagulability (min1: 6.48%/s vs 5.05%/s, P < 0.001; min2: 0.92%/s2 vs 0.74%/s2, P = 0.033). In conclusion, the thrombotic rates were low and did not differ between COVID-19 and non-CoV-2-RV patients. The hypercoagulability in COVID-19 is a highly dynamic process with the highest risk occurring when patients were most severely ill. Such changes in haemostasis could be detected by CWA. In our population, a more individualized thromboprophylaxis approach, considering clinical and laboratory factors, is preferred over universal pharmacological thromboprophylaxis for all hospitalized COVID-19 patients and such personalized approach warrants further research.
Conflict of interest statement
The authors declare no competing interests.
Figures
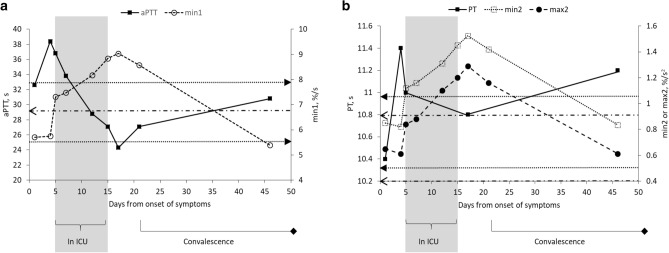
 ) depict the upper and lower limits of the reference intervals of aPTT while the horizontal dashed arrow (
) depict the upper and lower limits of the reference intervals of aPTT while the horizontal dashed arrow ( ) shows the upper limit of min1 reference interval (min1 lower limit falls below the boundary of the graph shown). (b) Serial PT, min2 and max2 data of the patient. All the PT results fall within the reference intervals of 9.9 s to 11.4 s. The horizontal dashed arrows (
) depict the upper and lower limits of the reference intervals of min2 while the horizontal dotted arrows (
) shows the upper limit of min1 reference interval (min1 lower limit falls below the boundary of the graph shown). (b) Serial PT, min2 and max2 data of the patient. All the PT results fall within the reference intervals of 9.9 s to 11.4 s. The horizontal dashed arrows (
) depict the upper and lower limits of the reference intervals of min2 while the horizontal dotted arrows ( ) show the upper and lower limits of max2 reference intervals. *Clinical deterioration defined as requiring intensive care unit (ICU) support
) show the upper and lower limits of max2 reference intervals. *Clinical deterioration defined as requiring intensive care unit (ICU) supportReferences
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
