

The importance of curve severity, type and instrumentation strategy in the surgical correction of adolescent idiopathic scoliosis: an in silico clinical trial on 64 cases
- PMID: 33469069
- PMCID: PMC7815774
- DOI: 10.1038/s41598-021-81319-z
The importance of curve severity, type and instrumentation strategy in the surgical correction of adolescent idiopathic scoliosis: an in silico clinical trial on 64 cases
Abstract
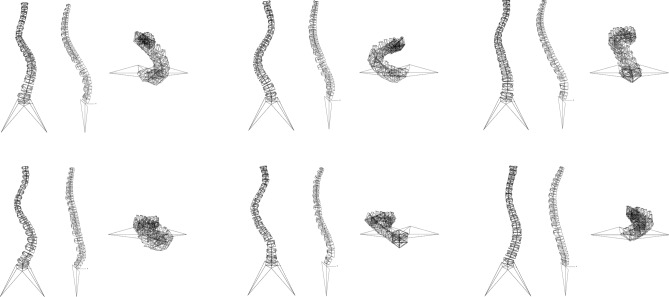
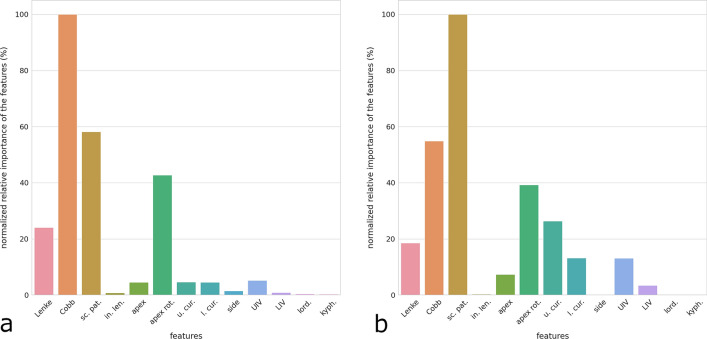
Adolescent idiopathic scoliosis is a three-dimensional deformity of the spine which is frequently corrected with the implantation of instrumentation with generally good or excellent clinical results; mechanical post-operative complications such as implant loosening and breakage are however relatively frequent. The rate of complications is associated with a lack of consensus about the surgical decision-making process; choices about the instrumentation length, the anchoring implants and the degree of correction are indeed mostly based on personal views and previous experience of the surgeon. In this work, we performed an in silico clinical trial on a large number of subjects in order to clarify which factors have the highest importance in determining the risk of complications by quantitatively analysing the mechanical stresses and loads in the instrumentation after the correction maneuvers. The results of the simulations highlighted the fundamental role of the curve severity, also in its three-dimensional aspect, and of the instrumentation strategy, whereas the length of the fixation had a lower importance.
Conflict of interest statement
The authors declare no competing interests.
Figures







References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
