

Differential relationships of PTSD symptom clusters with cortical thickness and grey matter volumes among women with PTSD
- PMID: 33469080
- PMCID: PMC7815843
- DOI: 10.1038/s41598-020-80776-2
Differential relationships of PTSD symptom clusters with cortical thickness and grey matter volumes among women with PTSD
Abstract
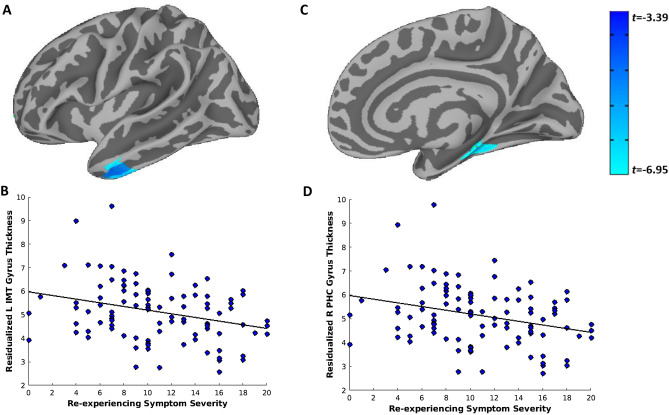
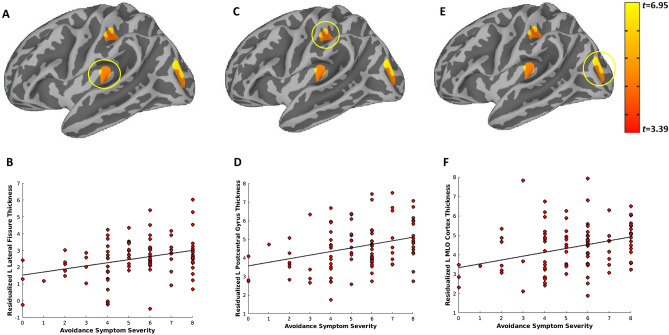
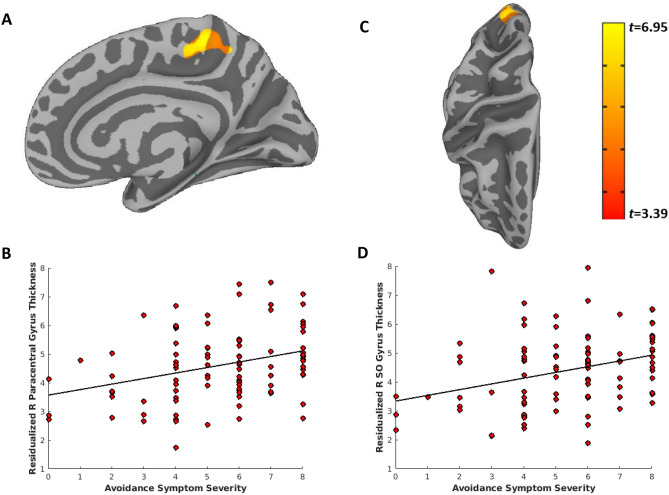
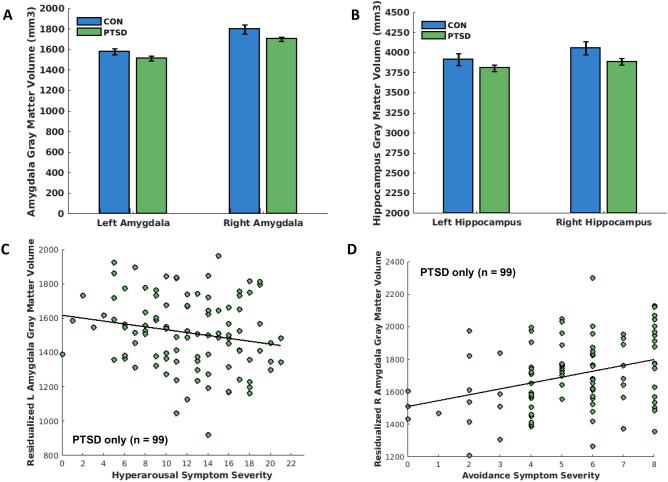
Structural neuroimaging studies of posttraumatic stress disorder (PTSD) have typically reported reduced cortical thickness (CT) and gray matter volume (GMV) in subcortical structures and networks involved in memory retrieval, emotional processing and regulation, and fear acquisition and extinction. Although PTSD is more common in women, and interpersonal violence (IPV) exposure is a more potent risk factor for developing PTSD relative to other forms of trauma, most of the existing literature examined combat-exposed men with PTSD. Vertex-wise CT and subcortical GMV analyses were conducted to examine potential differences in a large, well-characterized sample of women with PTSD stemming from IPV-exposure (n = 99) compared to healthy trauma-free women without a diagnosis of PTSD (n = 22). Subgroup analyses were also conducted to determine whether symptom severity within specific PTSD symptom clusters (e.g., re-experiencing, active avoidance, hyperarousal) predict CT and GMV after controlling for comorbid depression and anxiety. Results indicated that a diagnosis of PTSD in women with IPV-exposure did not significantly predict differences in CT across the cortex or GMV in the amygdala or hippocampus compared to healthy controls. However, within the PTSD group, greater re-experiencing symptom severity was associated with decreased CT in the left inferior and middle temporal gyrus, and decreased CT in the right parahippocampal and medial temporal gyrus. In contrast, greater active avoidance symptom severity was associated with greater CT in the left lateral fissure, postcentral gyrus, and middle/lateral occipital cortex, and greater CT in the right paracentral, posterior cingulate, and superior occipital gyrus. In terms of GMV, greater hyperarousal symptom severity was associated with reduced left amygdala GMV, while greater active avoidance symptom severity was associated with greater right amygdala GMV. These findings suggest that structural brain alterations among women with IPV-related PTSD may be driven by symptom severity within specific symptom clusters and that PTSD symptom clusters may have a differential (increased or decreased) association with brain structures.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- APA . Diagnostic and Statistical Manual of Mental Disorders. 5. Washington DC: APA; 2013.
-
- Kessler RC. Posttraumatic stress disorder: the burden to the individual and to society. J. Clin. Psychiatry. 2000;61(55):4–12. - PubMed
-
- Blanco, C. et al. Toward understanding sex differences in the prevalence of posttraumatic stress disorder: Results from the national epidemiologic survey on alcohol and related conditions. J. Clin. Psychiatry79 (2018). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
