

This is a preprint.
Differential T cell reactivity to seasonal coronaviruses and SARS-CoV-2 in community and health care workers
- PMID: 33469594
- PMCID: PMC7814840
- DOI: 10.1101/2021.01.12.21249683
Differential T cell reactivity to seasonal coronaviruses and SARS-CoV-2 in community and health care workers
Update in
-
Differential T-Cell Reactivity to Endemic Coronaviruses and SARS-CoV-2 in Community and Health Care Workers.J Infect Dis. 2021 Jul 2;224(1):70-80. doi: 10.1093/infdis/jiab176. J Infect Dis. 2021. PMID: 33822097 Free PMC article.
Abstract
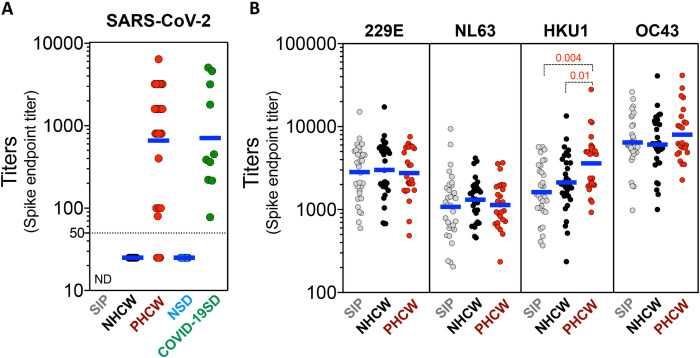
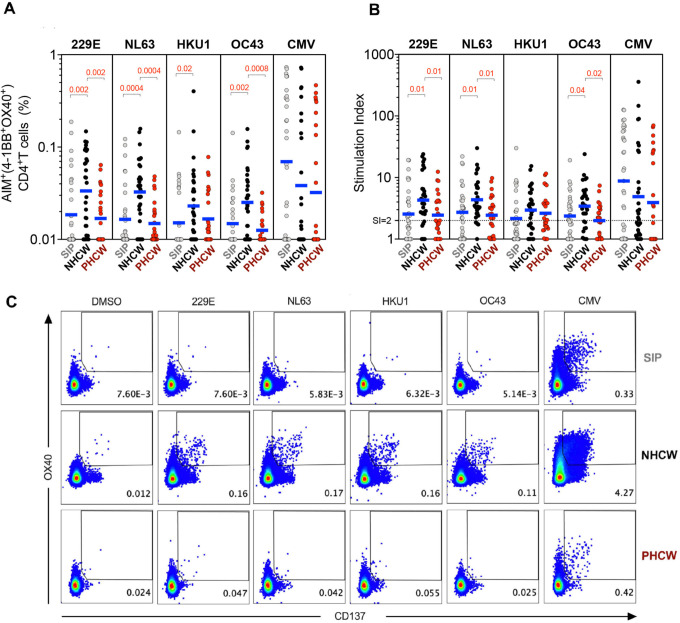
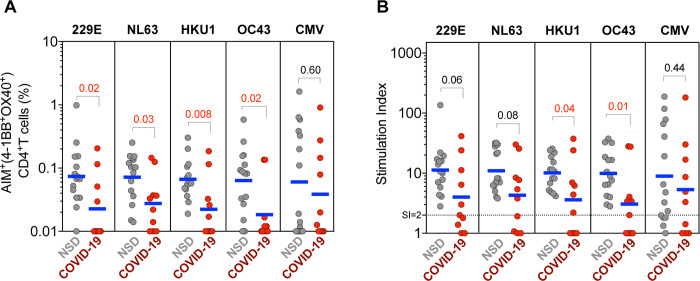
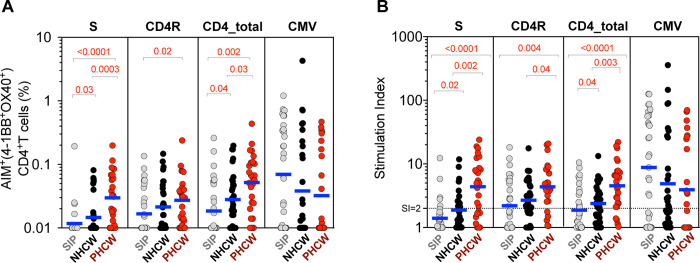
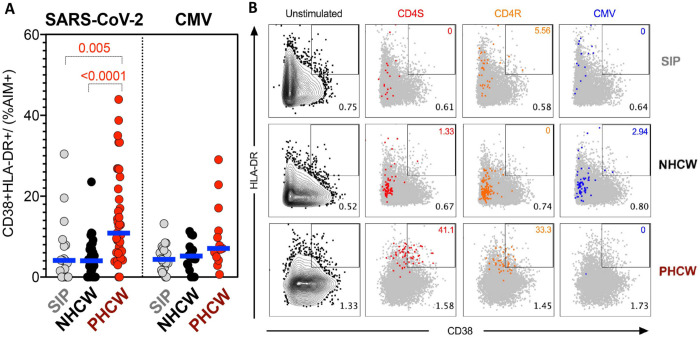
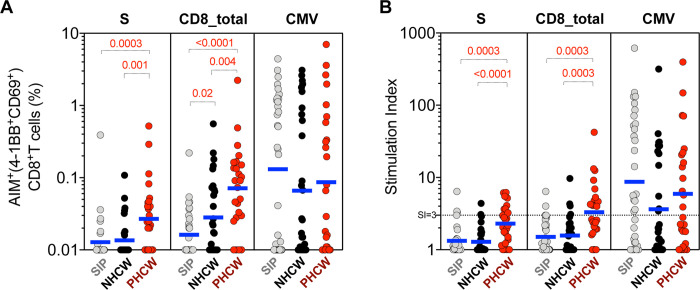
Herein we measured CD4+ T cell responses against common cold corona (CCC) viruses and SARS-CoV-2 in high-risk health care workers (HCW) and community controls. We observed higher levels of CCC reactive T cells in SARS-CoV-2 seronegative HCW compared to community donors, consistent with potential higher occupational exposure of HCW to CCC. We further show that SARS-CoV-2 reactivity of seronegative HCW was higher than community controls and correlation between CCC and SARS-CoV-2 responses is consistent with cross-reactivity and not associated with recent in vivo activation. Surprisingly, CCC reactivity was decreased in SARS-CoV-2 infected HCW, suggesting that exposure to SARS-CoV-2 might interfere with CCC responses, either directly or indirectly. This result was unexpected, but consistently detected in independent cohorts derived from Miami and San Diego.
Conflict of interest statement
Competing interests A.S. is a consultant for Gritstone, Flow Pharma, Merck, Epitogenesis, Gilead and Avalia. S.C. is a consultant for Avalia. LJI has filed for patent protection for various aspects of T cell epitope and vaccine design work. Mount Sinai has licensed serological assays to commercial entities and has filed for patent protection for serological assays. D.S., F.A., and F.K. are listed as inventors on the pending patent application (F.K.), and Newcastle disease virus (NDV)-based SARS-CoV-2 vaccines that name F.K. as inventor. Mount Sinai has licensed serological assays to commercial entities and has filed for patent protection for serological assays. D.S., F.A. and F.K. are listed as inventors on the pending patent application. All other authors declare no conflict of interest
Figures
Similar articles
-
Differential T-Cell Reactivity to Endemic Coronaviruses and SARS-CoV-2 in Community and Health Care Workers.J Infect Dis. 2021 Jul 2;224(1):70-80. doi: 10.1093/infdis/jiab176. J Infect Dis. 2021. PMID: 33822097 Free PMC article.
-
Evidence for broad cross-reactivity of the SARS-CoV-2 NSP12-directed CD4+ T-cell response with pre-primed responses directed against common cold coronaviruses.Front Immunol. 2023 May 5;14:1182504. doi: 10.3389/fimmu.2023.1182504. eCollection 2023. Front Immunol. 2023. PMID: 37215095 Free PMC article.
-
Immunopeptidome profiling of human coronavirus OC43-infected cells identifies CD4 T cell epitopes specific to seasonal coronaviruses or cross-reactive with SARS-CoV-2.bioRxiv [Preprint]. 2022 Dec 1:2022.12.01.518643. doi: 10.1101/2022.12.01.518643. bioRxiv. 2022. Update in: PLoS Pathog. 2023 Jul 27;19(7):e1011032. doi: 10.1371/journal.ppat.1011032. PMID: 36482973 Free PMC article. Updated. Preprint.
-
Immunological memory to Common Cold Coronaviruses assessed longitudinally over a three-year period.bioRxiv [Preprint]. 2022 Mar 2:2022.03.01.482548. doi: 10.1101/2022.03.01.482548. bioRxiv. 2022. Update in: Cell Host Microbe. 2022 Sep 14;30(9):1269-1278.e4. doi: 10.1016/j.chom.2022.07.012. PMID: 35262082 Free PMC article. Updated. Preprint.
-
Exposed seronegative: Cellular immune responses to SARS-CoV-2 in the absence of seroconversion.Front Immunol. 2023 Jan 26;14:1092910. doi: 10.3389/fimmu.2023.1092910. eCollection 2023. Front Immunol. 2023. PMID: 36776841 Free PMC article. Review.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous