

Association of Lipid, Inflammatory, and Metabolic Biomarkers With Age at Onset for Incident Coronary Heart Disease in Women
- PMID: 33471027
- PMCID: PMC7818181
- DOI: 10.1001/jamacardio.2020.7073
Association of Lipid, Inflammatory, and Metabolic Biomarkers With Age at Onset for Incident Coronary Heart Disease in Women
Abstract
Importance: Risk profiles for premature coronary heart disease (CHD) are unclear.
Objective: To examine baseline risk profiles for incident CHD in women by age at onset.
Design, setting, and participants: A prospective cohort of US female health professionals participating in the Women's Health Study was conducted; median follow-up was 21.4 years. Participants included 28 024 women aged 45 years or older without known cardiovascular disease. Baseline profiles were obtained from April 30, 1993, to January 24, 1996, and analyses were conducted from October 1, 2017, to October 1, 2020.
Exposures: More than 50 clinical, lipid, inflammatory, and metabolic risk factors and biomarkers.
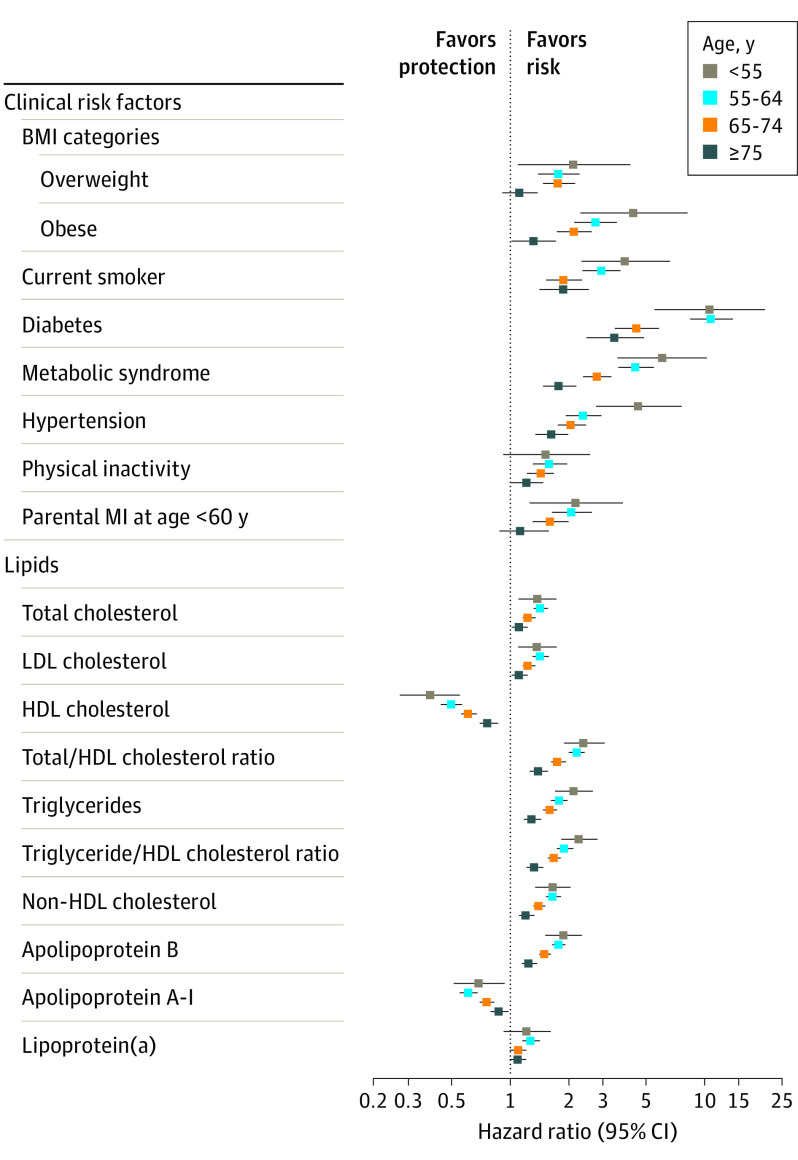
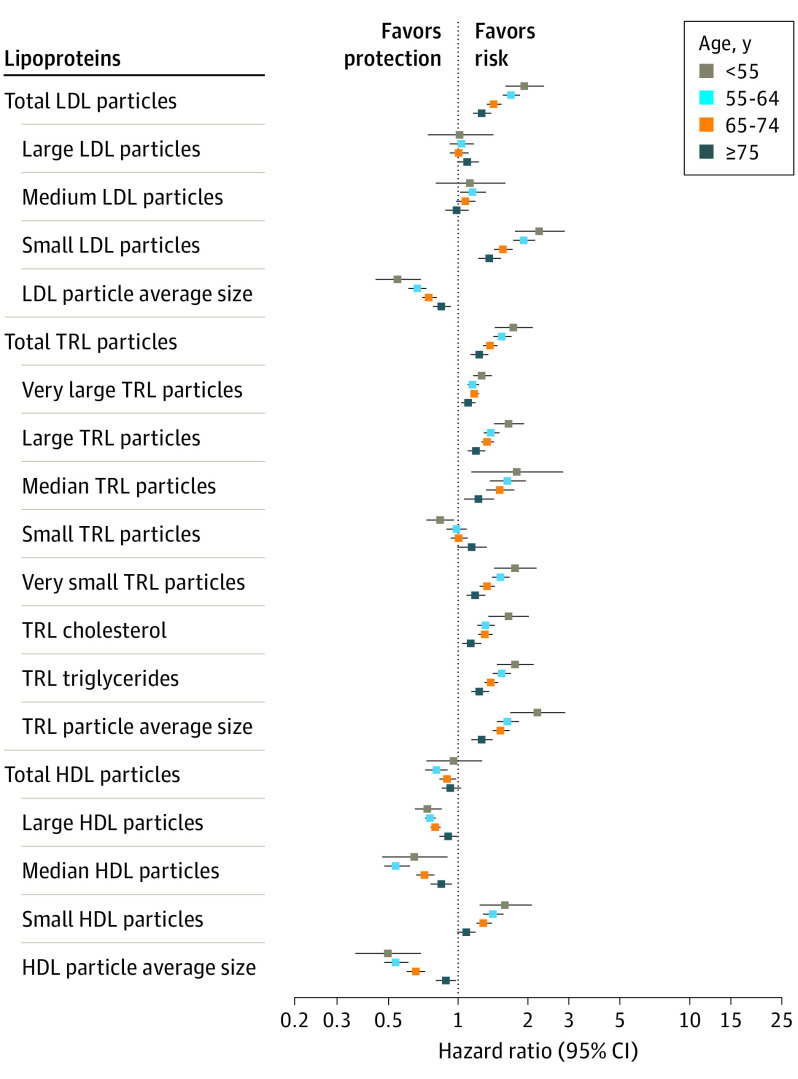
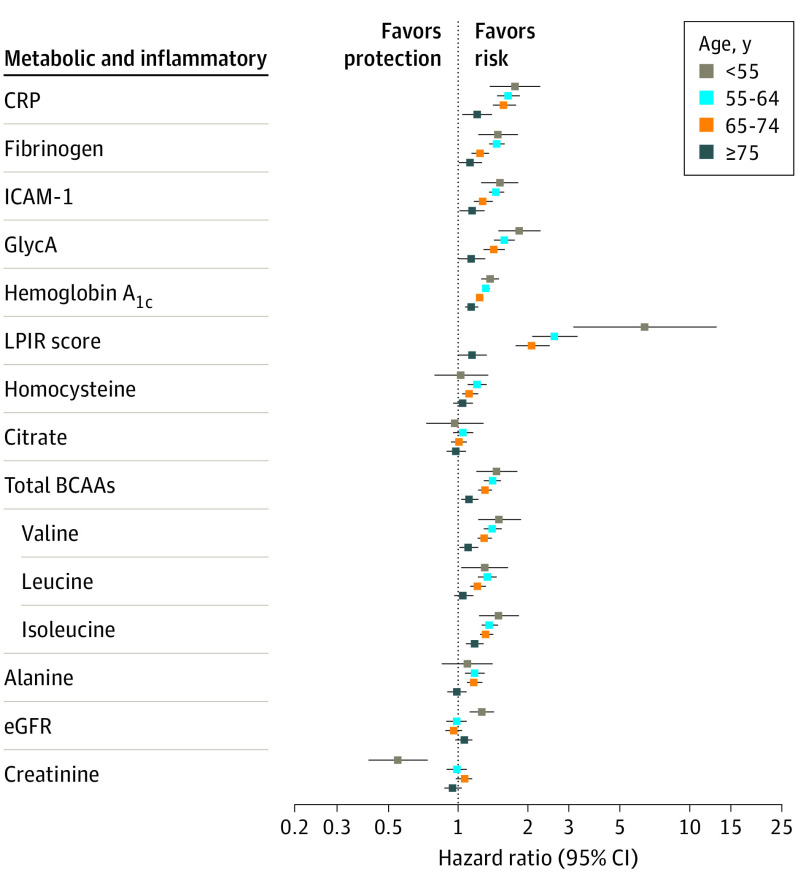
Main outcomes and measures: Four age groups were examined (<55, 55 to <65, 65 to <75, and ≥75 years) for CHD onset, and adjusted hazard ratios (aHRs) were calculated using stratified Cox proportional hazard regression models with age as the time scale and adjusting for clinical factors. Women contributed to different age groups over time.
Results: Of the clinical factors in the women, diabetes had the highest aHR for CHD onset at any age, ranging from 10.71 (95% CI, 5.57-20.60) at CHD onset in those younger than 55 years to 3.47 (95% CI, 2.47-4.87) at CHD onset in those 75 years or older. Risks that were also noted for CHD onset in participants younger than 55 years included metabolic syndrome (aHR, 6.09; 95% CI, 3.60-10.29), hypertension (aHR, 4.58; 95% CI, 2.76-7.60), obesity (aHR, 4.33; 95% CI, 2.31-8.11), and smoking (aHR, 3.92; 95% CI, 2.32-6.63). Myocardial infarction in a parent before age 60 years was associated with 1.5- to 2-fold risk of CHD in participants up to age 75 years. From approximately 50 biomarkers, lipoprotein insulin resistance had the highest standardized aHR: 6.40 (95% CI, 3.14-13.06) for CHD onset in women younger than 55 years, attenuating with age. In comparison, weaker but significant associations with CHD in women younger than 55 years were noted (per SD increment) for low-density lipoprotein cholesterol (aHR, 1.38; 95% CI, 1.10-1.74), non-high-density lipoprotein cholesterol (aHR, 1.67; 95% CI, 1.36-2.04), apolipoprotein B (aHR, 1.89; 95% CI, 1.52-2.35), triglycerides (aHR, 2.14; 95% CI, 1.72-2.67), and inflammatory biomarkers (1.2- to 1.8-fold)-all attenuating with age. Some biomarkers had similar CHD age associations (eg, physical inactivity, lipoprotein[a], total high-density lipoprotein particles), while a few had no association with CHD onset at any age. Most risk factors and biomarkers had associations that attenuated with increasing age at onset.
Conclusions and relevance: In this cohort study, diabetes and insulin resistance, in addition to hypertension, obesity, and smoking, appeared to be the strongest risk factors for premature onset of CHD. Most risk factors had attenuated relative rates at older ages.
Conflict of interest statement
Figures
References
-
- De Sutter J, De Bacquer D, Kotseva K, et al. ; EUROpean Action on Secondary Prevention through Intervention to Reduce Events II study group . Screening of family members of patients with premature coronary heart disease; results from the EUROASPIRE II family survey. Eur Heart J. 2003;24(3):249-257. doi: 10.1016/S0195-668X(02)00386-X - DOI - PubMed
-
- Kotseva K, Wood D, De Backer G, De Bacquer D, Pyörälä K, Keil U; EUROASPIRE Study Group . EUROASPIRE III: a survey on the lifestyle, risk factors and use of cardioprotective drug therapies in coronary patients from 22 European countries. Eur J Cardiovasc Prev Rehabil. 2009;16(2):121-137. doi: 10.1097/HJR.0b013e3283294b1d - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
