

Effectiveness of Systematic Echocardiographic Screening for Rheumatic Heart Disease in Nepalese Schoolchildren: A Cluster Randomized Clinical Trial
- PMID: 33471029
- PMCID: PMC7818193
- DOI: 10.1001/jamacardio.2020.7050
Effectiveness of Systematic Echocardiographic Screening for Rheumatic Heart Disease in Nepalese Schoolchildren: A Cluster Randomized Clinical Trial
Abstract
Importance: Echocardiographic screening allows for early detection of subclinical stages of rheumatic heart disease among children in endemic regions.
Objective: To investigate the effectiveness of systematic echocardiographic screening in combination with secondary antibiotic prophylaxis on the prevalence of rheumatic heart disease.
Design, setting, and participants: This cluster randomized clinical trial included students 9 to 16 years of age attending public and private schools in urban and rural areas of the Sunsari district in Nepal that had been randomly selected on November 17, 2012. Echocardiographic follow-up was performed between January 7, 2016, and January 3, 2019.
Interventions: In the experimental group, children underwent systematic echocardiographic screening followed by secondary antibiotic prophylaxis in case they had echocardiographic evidence of latent rheumatic heart disease. In the control group, children underwent no echocardiographic screening.
Main outcomes and measures: Prevalence of the composite of definite or borderline rheumatic heart disease according to the World Heart Federation criteria in experimental and control schools as assessed 4 years after intervention.
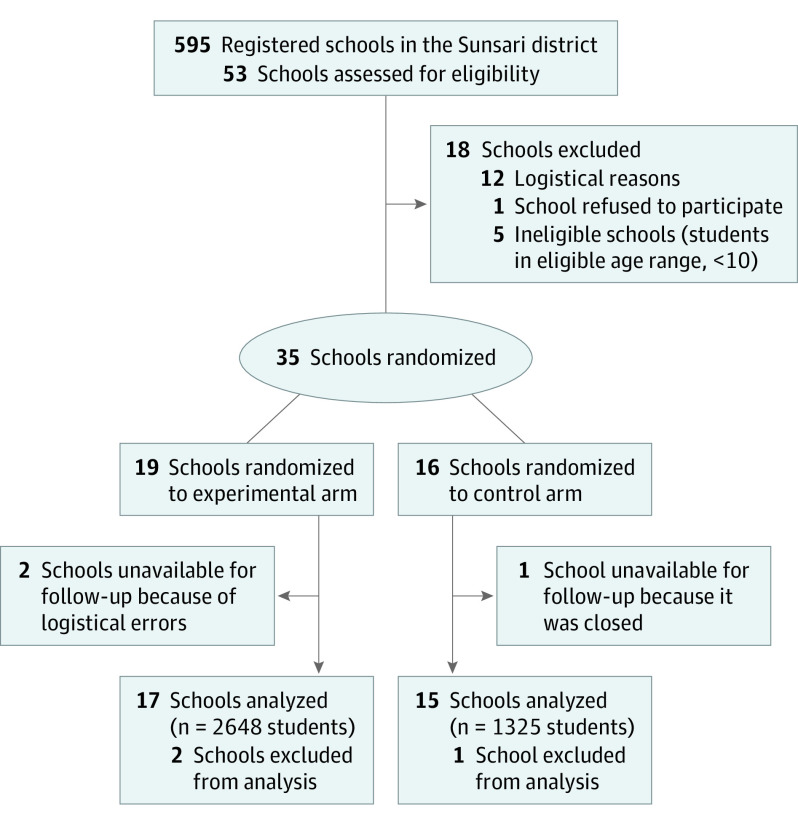
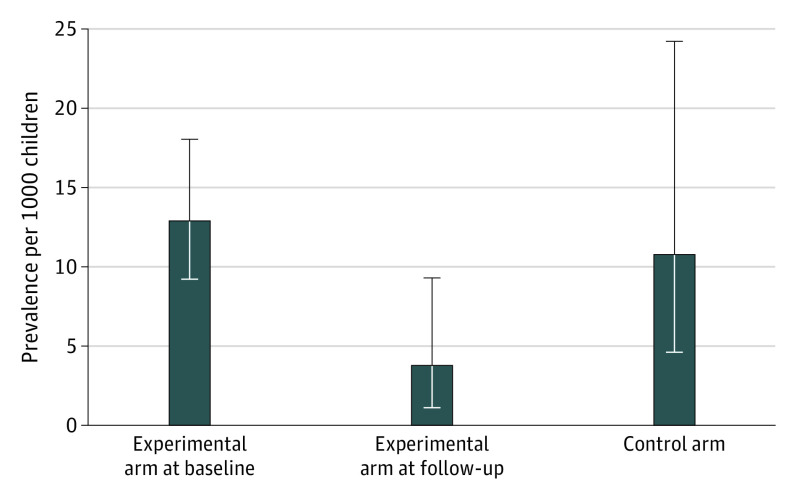
Results: A total of 35 schools were randomized to the experimental group (n = 19) or the control group (n = 16). After a median of 4.3 years (interquartile range [IQR], 4.0-4.5 years), 17 of 19 schools in the experimental group (2648 children; median age at follow-up, 12.1 years; IQR, 10.3-12.5 years; 1308 [49.4%] male) and 15 of 16 schools in the control group (1325 children; median age at follow-up, 10.6 years; IQR, 10.0-12.5 years; 682 [51.5%] male) underwent echocardiographic follow-up. The prevalence of definite or borderline rheumatic heart disease was 10.8 per 1000 children (95% CI, 4.7-24.7) in the control group and 3.8 per 1000 children (95% CI, 1.5-9.8) in the experimental group (odds ratio, 0.34; 95% CI, 0.11-1.07; P = .06). The prevalence in the experimental group at baseline had been 12.9 per 1000 children (95% CI, 9.2-18.1). In the experimental group, the odds ratio of definite or borderline rheumatic heart disease at follow-up vs baseline was 0.29 (95% CI, 0.13-0.65; P = .008).
Conclusions and relevance: School-based echocardiographic screening in combination with secondary antibiotic prophylaxis in children with evidence of latent rheumatic heart disease may be an effective strategy to reduce the prevalence of definite or borderline rheumatic heart disease in endemic regions.
Trial registration: ClinicalTrials.gov Identifier: NCT01550068.
Conflict of interest statement
Figures
Comment in
-
Screening for Rheumatic Heart Disease-Quo Vadis?JAMA Cardiol. 2021 Apr 1;6(4):375-376. doi: 10.1001/jamacardio.2020.7063. JAMA Cardiol. 2021. PMID: 33471062 No abstract available.
References
-
- Yadgir S, Johnson CO, Aboyans V, et al. ; Global Burden of Disease Study 2017 Nonrheumatic Valve Disease Collaborators . Global, regional, and national burden of calcific aortic valve and degenerative mitral valve diseases, 1990-2017. Circulation. 2020;141(21):1670-1680. doi: 10.1161/CIRCULATIONAHA.119.043391 - DOI - PubMed
-
- World Health Organization Study Group on Rheumatic Fever and Heart Disease . Rheumatic fever and rheumatic heart disease: report of a WHO expert consultation, Geneva, 20 October - 1 November 2001. 2004. https://apps.who.int/iris/handle/10665/42898
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
