

Implementation of the acutely presenting older patient (APOP) screening program in routine emergency department care : A before-after study
- PMID: 33471176
- PMCID: PMC7946672
- DOI: 10.1007/s00391-020-01837-9
Implementation of the acutely presenting older patient (APOP) screening program in routine emergency department care : A before-after study
Abstract
Objective: The aim of this study was to evaluate the effects of implementation of the acutely presenting older patient (APOP) screening program for older patients in routine emergency department (ED) care shortly after implementation.
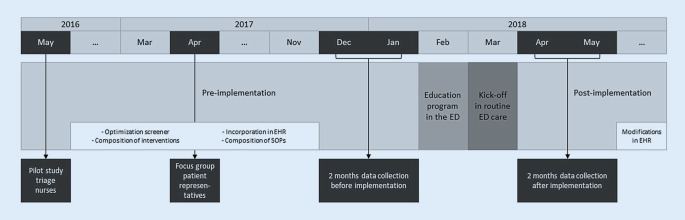
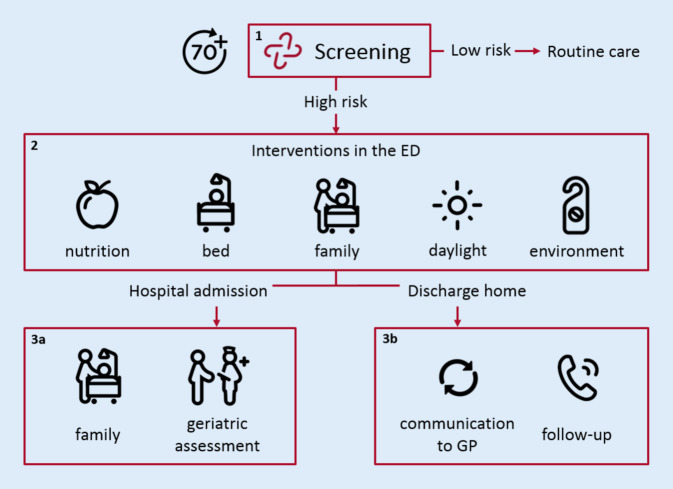
Methods: We conducted an implementation study with before-after design, using the plan-do-study-act (PDSA) model for quality improvement, in the ED of a Dutch academic hospital. All consecutive patients ≥ 70 years during 2 months before and after implementation were included. The APOP program comprises screening for risk of functional decline, mortality and cognitive impairment, targeted interventions for high-risk patients and education of professionals. Outcome measures were compliance with interventions and impact on ED process, length of stay (LOS) and hospital admission rate.
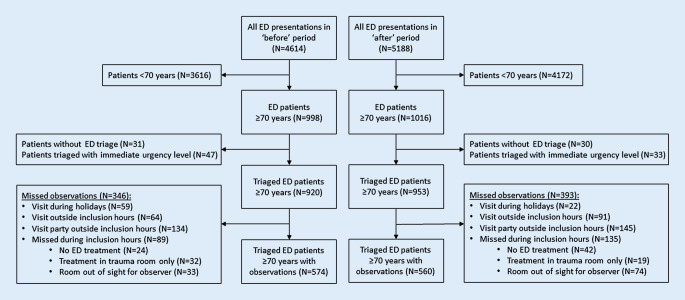
Results: Two comparable groups of patients (median age 77 years) were included before (n = 920) and after (n = 953) implementation. After implementation 560 (59%) patients were screened of which 190 (34%) were high-risk patients. Some of the program interventions for high-risk patients in the ED were adhered to, some were not. More hospitalized patients received comprehensive geriatric assessment (CGA) after implementation (21% before vs. 31% after; p = 0.002). In 89% of high-risk patients who were discharged to home, telephone follow-up was initiated. Implementation did not influence median ED LOS (202 min before vs. 196 min after; p = 0.152) or hospital admission rate (40% before vs. 39% after; p = 0.410).
Conclusion: Implementation of the APOP screening program in routine ED care did not negatively impact the ED process and resulted in an increase of CGA and telephone follow-up in older patients. Future studies should investigate whether sustainable changes in management and patient outcomes occur after more PDSA cycles.
Zusammenfassung: ZIELSETZUNG: Beurteilung der Auswirkungen der Implementierung des Screening-Programms für ältere Patienten (APOP) in der Routineversorgung der Notaufnahme (ED) kurz nach der Anwendung.
Methoden: Eine Implementierungsstudie mit Vorher-Nachher-Design wurde unter Verwendung des Plan-do-study-act(PDSA)-Modells zur Qualitätsverbesserung in der Notaufnahme eines niederländischen akademischen Krankenhauses durchgeführt. Alle konsekutiven Patienten ≥70 Jahre während der 2 Monate vor und nach der Implementierung wurden eingeschlossen. Das APOP-Screening-Programm umfasst eine Untersuchung auf das Risiko von Funktionseinschränkungen, Mortalität und kognitiver Beeinträchtigung, gezielte Interventionen für Hochrisikopatienten und die Schulung von Fachpersonal. Die Ergebnisse wurden anhand der Compliance mit den Interventionen und den Auswirkungen auf die Abläufe in der Notaufnahme, die Verweildauer (LOS) und die Krankenhauseinweisungsrate gemessen.
Ergebnisse: Zwei vergleichbare Gruppen von Patienten (mittleres Alter: 77 Jahre) wurden vor (n = 920) und nach (n = 953) der Implementierung eingeschlossen. Nach der Implementierung wurden 560 (59 %) Patienten gescreent, von denen 190 (34 %) Hochrisikopatienten waren. Die Interventionen für Hochrisikopatienten in der Notaufnahme wurden teilweise eingehalten. Mehr hospitalisierte Patienten erhielten nach der Implementierung ein umfassendes geriatrisches Assessment (CGA; 21 % vorher vs. 31 % nachher; p = 0,002). Bei 89 % der Hochrisikopatienten, die nach Hause entlassen wurden, wurde eine telefonische Nachbetreuung eingeleitet. Die Implementierung hatte keinen Einfluss auf die mediane Verweildauer in der Notaufnahme (202 min vorher vs. 196 min nachher; p = 0,152) oder die Krankenhauseinweisungsrate (40 % vorher vs. 39 % nachher; p = 0,410).
Schlussfolgerung: Die Implementierung des APOP-Screening-Programms in die routinemäßige Versorgung in der Notaufnahme hatte keine negativen Auswirkungen auf den ED-Prozess und führte zu einer Zunahme von CGA und telefonischer Nachsorge bei älteren Patienten. In zukünftigen Studien sollte untersucht werden, ob nach weiteren PDSA-Zyklen nachhaltige Veränderungen im Management und in den Patientenergebnissen auftreten.
Keywords: Frail elderly; Geriatric assessment; Geriatric emergency medicine; Implementation science; Quality improvement.
Conflict of interest statement
L.C. Blomaard, B. de Groot, J.A. Lucke, J. de Gelder, A.M. Booijen, J. Gussekloo and S.P. Mooijaart declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
