

The prevalence and clinical outcome of supraventricular tachycardia in different etiologies of pulmonary hypertension
- PMID: 33471824
- PMCID: PMC7817034
- DOI: 10.1371/journal.pone.0245752
The prevalence and clinical outcome of supraventricular tachycardia in different etiologies of pulmonary hypertension
Abstract
Purpose: Patients with pulmonary hypertension (PH) frequently suffer from supraventricular tachycardias (SVT). The main purpose of our study was to identify the cumulative incidence of SVT in patients with different etiologies of PH. The secondary objective was to analyse the clinical impact of SVT.
Methods: We retrospectively studied the prevalence of SVT and the clinical outcome in 755 patients (41% males; 60 ± 15 years; mean follow-up 3.8 ± 2.8 years) with PH of different etiologies. The prevalence of SVT was analysed separately in isolated pre-capillary PH (Ipc-PH) and in patients with combined post- and pre-capillary PH (Cpc-PH).
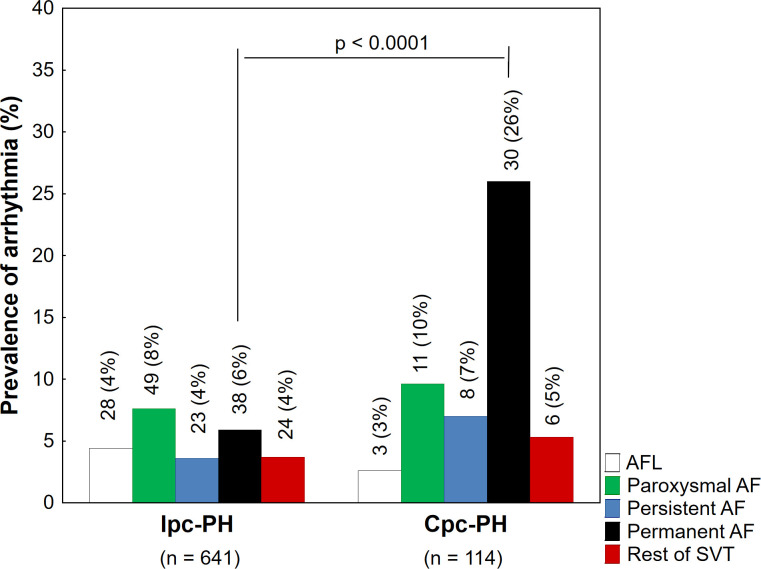
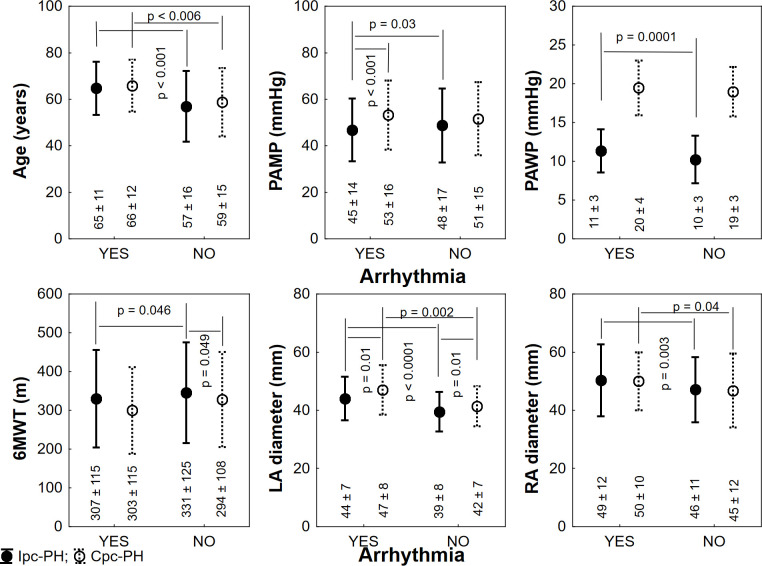
Results: The prevalence of SVT in the Ipc-PH group (n = 641) was 25% (n = 162). The most prevalent arrhythmias were atrial fibrillation followed by a typical atrial flutter (17% and 4.4% of all Icp-PH patients). An excessive prevalence of SVT was found in patients with pulmonary arterial hypertension associated with congenital heart disease (35%, p = 0.01). Out of the overall study population, Cpc-PH was present in 114 (15%) patients. Patients with Cpc-PH manifested a higher prevalence of SVT than subjects with Ipc-PH (58; 51% vs. 162; 25%; p <0.0001) and were more likely to have persistent or permanent atrial fibrillation (38; 29% vs. 61; 10%; p <0.0001). Parameters significantly associated with mortality in a multivariate analysis included age, male gender, functional exercise capacity and right atrial diameter (p < 0.05). Neither diagnosis of SVT nor type of arrhythmia predicted mortality.
Conclusions: The study detected a significant prevalence of SVT in the population of PH of different origins. Different spectrum and prevalence of arrhythmia might be expected in different etiologies of PH. Patients with an elevated post-capillary pressure showed a higher arrhythmia prevalence, predominantly due to an excessive number of atrial fibrillations. The diagnosis of SVT was not associated with mortality.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Incidence and clinical relevance of supraventricular tachyarrhythmias in pulmonary hypertension.Am Heart J. 2007 Jan;153(1):127-32. doi: 10.1016/j.ahj.2006.09.008. Am Heart J. 2007. PMID: 17174650
-
The left atrial substrate plays a significant role in the development of complex atrial tachycardia in patients with precapillary pulmonary hypertension.BMC Cardiovasc Disord. 2019 Jun 28;19(1):157. doi: 10.1186/s12872-019-1142-z. BMC Cardiovasc Disord. 2019. PMID: 31253083 Free PMC article.
-
Long term prognosis in patients with pulmonary hypertension undergoing catheter ablation for supraventricular tachycardia.Sci Rep. 2021 Aug 10;11(1):16176. doi: 10.1038/s41598-021-95508-3. Sci Rep. 2021. PMID: 34376719 Free PMC article.
-
[How to approach the patient with supraventricular tachycardia in the EP lab: A systematic overview].Herzschrittmacherther Elektrophysiol. 2015 Jun;26(2):167-72. doi: 10.1007/s00399-015-0373-7. Epub 2015 Jun 2. Herzschrittmacherther Elektrophysiol. 2015. PMID: 26031513 Review. German.
-
Interventional electrophysiology and its role in the treatment of cardiac arrhythmia.Ann Acad Med Singap. 1998 Mar;27(2):248-54. Ann Acad Med Singap. 1998. PMID: 9663319 Review.
Cited by
-
Incidence and prognostic significance of malignant arrhythmias during (repetitive) Holter electrocardiograms in patients with pulmonary hypertension.Front Cardiovasc Med. 2023 Apr 17;10:1084051. doi: 10.3389/fcvm.2023.1084051. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37139131 Free PMC article.
-
Radiofrequency catheter ablation for pulmonary hypertension patients with atrial flutter.ESC Heart Fail. 2024 Apr;11(2):883-892. doi: 10.1002/ehf2.14659. Epub 2024 Jan 10. ESC Heart Fail. 2024. PMID: 38200382 Free PMC article.
-
New-Onset Atrial Fibrillation Following Isolated Coronary Artery Bypass Grafting: Is Pulmonary Hypertension a Risk Factor?Braz J Cardiovasc Surg. 2025 Aug 26;40(5):e20240352. doi: 10.21470/1678-9741-2024-0352. Braz J Cardiovasc Surg. 2025. PMID: 40857580 Free PMC article.
-
Association Between the Coronary Sinus Ostial Size and Atrioventricular Nodal Reentrant Tachycardia in Patients With Pulmonary Arterial Hypertension.Front Physiol. 2022 Jan 21;12:790077. doi: 10.3389/fphys.2021.790077. eCollection 2021. Front Physiol. 2022. PMID: 35126179 Free PMC article.
-
The spectrum and prevalence of arrhythmia in different clinical pulmonary hypertension groups in Chinese population.Clin Cardiol. 2022 May;45(5):495-502. doi: 10.1002/clc.23803. Epub 2022 Mar 7. Clin Cardiol. 2022. PMID: 35253244 Free PMC article.
References
-
- Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016;37(1):67–119. 10.1093/eurheartj/ehv317 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
