

Clinical characteristics of treatment-resistant depression in adults in Hungary: Real-world evidence from a 7-year-long retrospective data analysis
- PMID: 33471854
- PMCID: PMC7817060
- DOI: 10.1371/journal.pone.0245510
Clinical characteristics of treatment-resistant depression in adults in Hungary: Real-world evidence from a 7-year-long retrospective data analysis
Abstract
Purpose: Treatment-resistant depression (TRD) is associated with a poor quality of life and high economic burden. This observational retrospective epidemiological study aimed to estimate the proportion of patients with TRD within a cohort of patients with major depressive disorder (MDD) in Hungary and examine the mortality and comorbidities of patients with and without TRD.
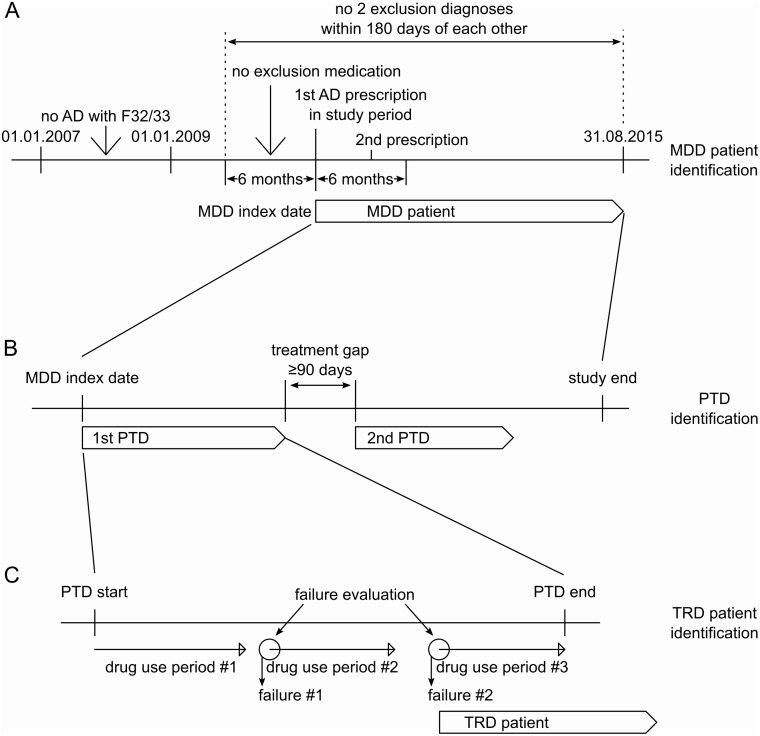
Patients and methods: This study included patients with MDD who experienced onset of a new depressive episode between 01 January 2009 and 31 August 2015, using data from a nationwide, longitudinal database.
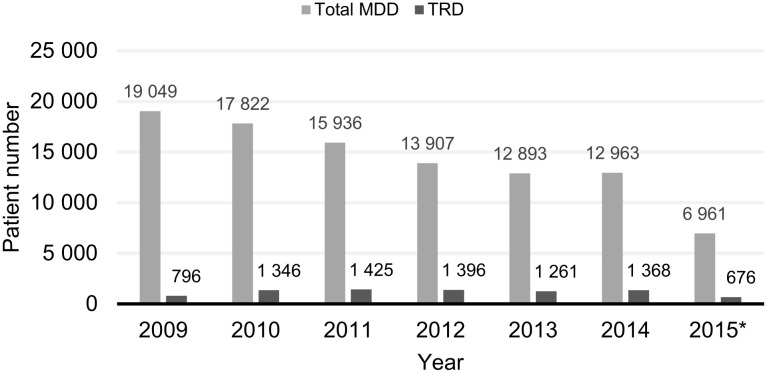
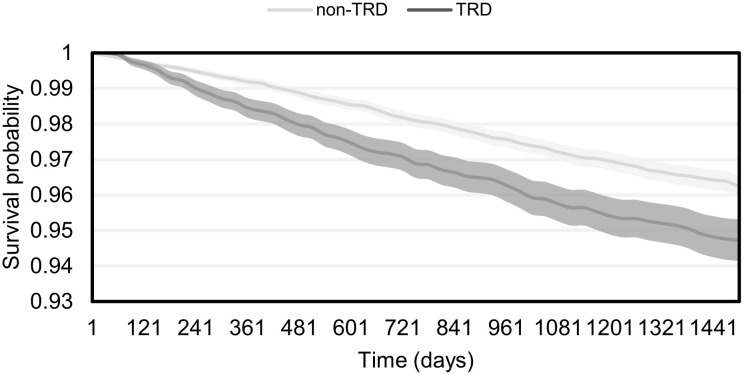
Results: Overall, 99,531 patients were included in the MDD cohort, of which 8,268 (8.3%) also met the criteria for TRD. The overall survival of non-TRD patients was longer than in TRD patients; the risk of mortality for TRD patients was significantly higher than of non-TRD patients (HR [CI] 1.381 [1.212-1.571]; p<0.001). Patients with TRD had a significantly higher probability of having "Neurotic, stress-related and somatoform disordersˮ, autoimmune conditions, cardio- or cerebrovascular diseases, thyroid gland diseases and self-harming behaviour not resulting in death than non-TRD patients (for all comparisons, p values were less than 0.005).
Discussion: To our best knowledge, this is the first study to assess the frequency of TRD in Hungary. In a cohort of Hungarian MDD patients, we have found that the proportion of TRD (~8.3%) is comparable to those reported in previous studies with similar methodology from other countries. The majority of our other main findings (e.g. more frequent self-harming behaviour, increased risk of "Neurotic, stress-related and somatoform disordersˮ and higher overall mortality in TRD subjects) are also in line with previous results from other countries. Taking the substantial proportion of patients with TRD into consideration, a more comprehensive and targeted treatment strategy would be required for these individuals.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: PK, LF, SMH and SB are employees of Janssen. PT was formerly an employee of Janssen. TB, KD are employees of Healthware Ltd., which company received funding from Janssen for the participation in the study. PD received fees for consultancy from Janssen. ZR received fees for consultancy from Janssen, received speaker’s honoraria from Janssen, Servier and Krka, and served as an advisory board member for Lundbeck, Janssen, Servier and Krka. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Economic impact of treatment-resistant depression: A retrospective observational study.J Affect Disord. 2021 Dec 1;295:578-586. doi: 10.1016/j.jad.2021.08.036. Epub 2021 Aug 27. J Affect Disord. 2021. PMID: 34509073
-
An Evaluation of the Clinical and Economic Burden Among Older Adult Medicare-Covered Beneficiaries With Treatment-Resistant Depression.Am J Geriatr Psychiatry. 2020 Mar;28(3):350-362. doi: 10.1016/j.jagp.2019.10.012. Epub 2019 Oct 22. Am J Geriatr Psychiatry. 2020. PMID: 31735488
-
Epidemiology of treatment resistant depression among major depressive disorder patients in Israel.BMC Psychiatry. 2022 Aug 11;22(1):541. doi: 10.1186/s12888-022-04184-8. BMC Psychiatry. 2022. PMID: 35948895 Free PMC article.
-
The burden of treatment-resistant depression: A systematic review of the economic and quality of life literature.J Affect Disord. 2019 Jan 1;242:195-210. doi: 10.1016/j.jad.2018.06.045. Epub 2018 Jun 27. J Affect Disord. 2019. PMID: 30195173
-
The contribution of polyamine pathway to determinations of diagnosis for treatment-resistant depression: A metabolomic analysis.Prog Neuropsychopharmacol Biol Psychiatry. 2024 Jan 10;128:110849. doi: 10.1016/j.pnpbp.2023.110849. Epub 2023 Sep 1. Prog Neuropsychopharmacol Biol Psychiatry. 2024. PMID: 37659714 Review.
Cited by
-
Cardiovascular Risk Predicts White Matter Hyperintensities, Brain Atrophy and Treatment Resistance in Major Depressive Disorder: Role of Genetic Liability.Acta Psychiatr Scand. 2025 Jun;151(6):709-718. doi: 10.1111/acps.13793. Epub 2025 Feb 27. Acta Psychiatr Scand. 2025. PMID: 40014927 Free PMC article.
-
Clinical and Biological Factors Are Associated with Treatment-Resistant Depression.Behav Sci (Basel). 2022 Feb 3;12(2):34. doi: 10.3390/bs12020034. Behav Sci (Basel). 2022. PMID: 35200285 Free PMC article.
-
Treatment-Resistant Depression in Poland-Epidemiology and Treatment.J Clin Med. 2022 Jan 18;11(3):480. doi: 10.3390/jcm11030480. J Clin Med. 2022. PMID: 35159935 Free PMC article.
-
The Individual and Societal Burden of Treatment-Resistant Depression: An Overview.Psychiatr Clin North Am. 2023 Jun;46(2):211-226. doi: 10.1016/j.psc.2023.02.001. Psychiatr Clin North Am. 2023. PMID: 37149341 Free PMC article. Review.
-
Study to determine the epidemiology of treatment-resistant depression among the Saudi Arabian population: A cross-sectional study.J Educ Health Promot. 2024 Jan 22;12:425. doi: 10.4103/jehp.jehp_809_23. eCollection 2023. J Educ Health Promot. 2024. PMID: 38464636 Free PMC article.
References
-
- Merikangas K, Rihmer Z. Mood Disorders: Epidemiology In: Sadock BJ, S V, Ruiz P, editor. Kaplan & Sadock’s Comprehensive Textbook of Psychiatry. 10th ed Philadelphia, USA: Wolters Kluwer; 2017. p. 1614–9.
-
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. Geneva, Switzerland: World Health Organization; 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
