

Automated Apnea-Hypopnea Index from Oximetry and Spectral Analysis of Cardiopulmonary Coupling
- PMID: 33472017
- PMCID: PMC12038919
- DOI: 10.1513/AnnalsATS.202005-510OC
Automated Apnea-Hypopnea Index from Oximetry and Spectral Analysis of Cardiopulmonary Coupling
Abstract
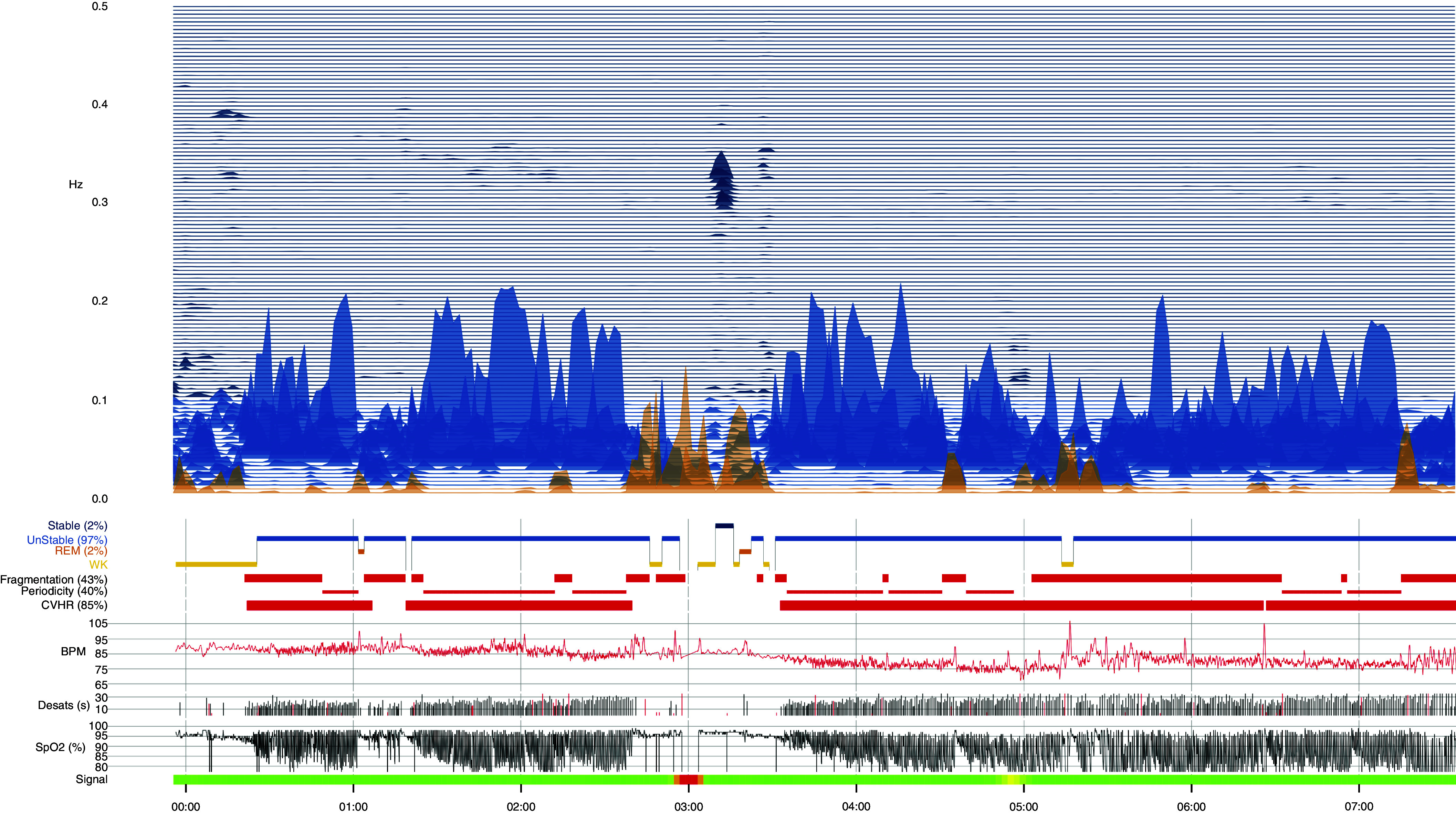
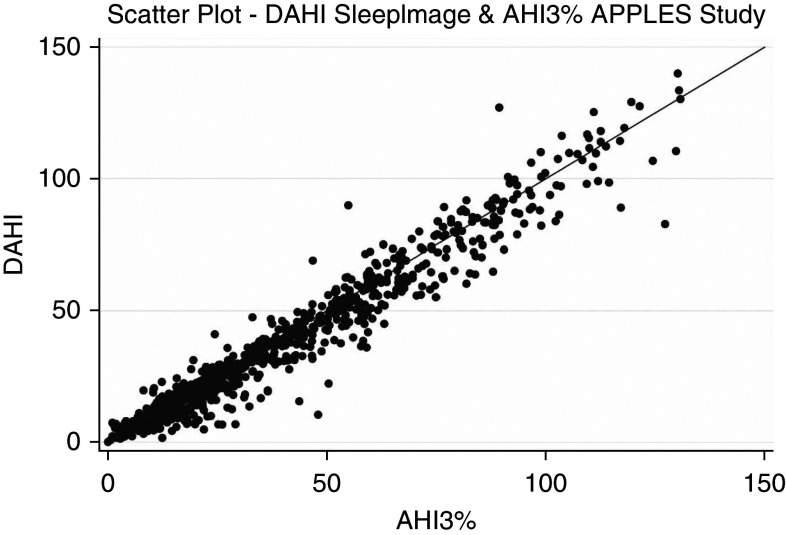
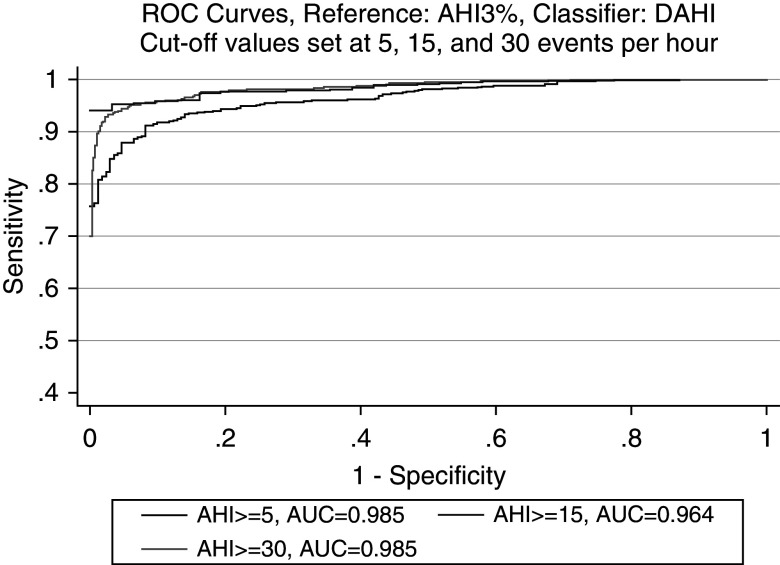
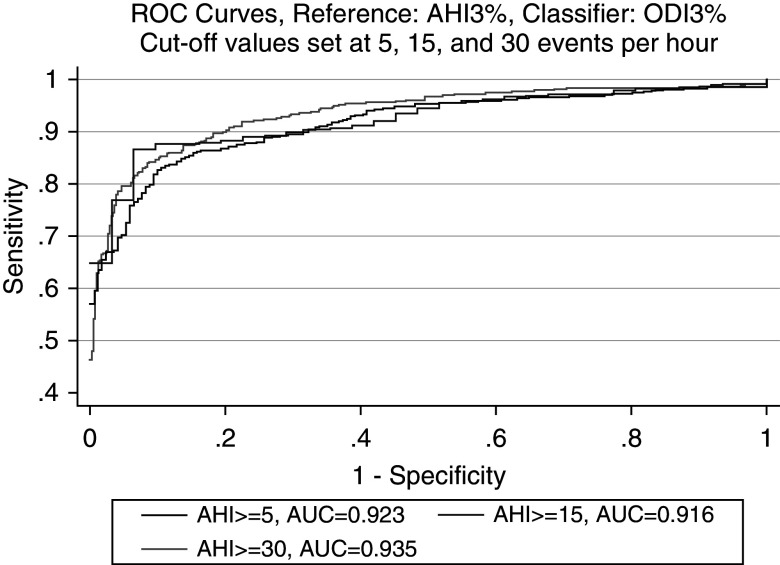
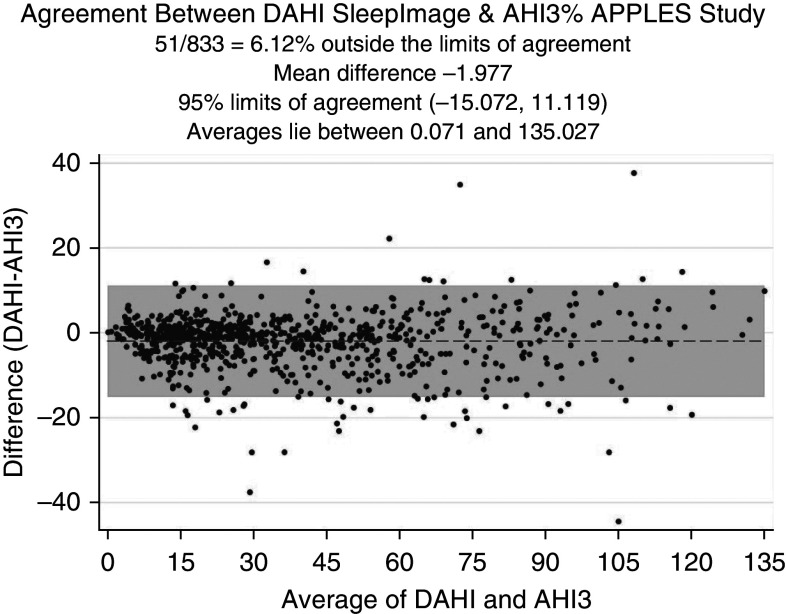
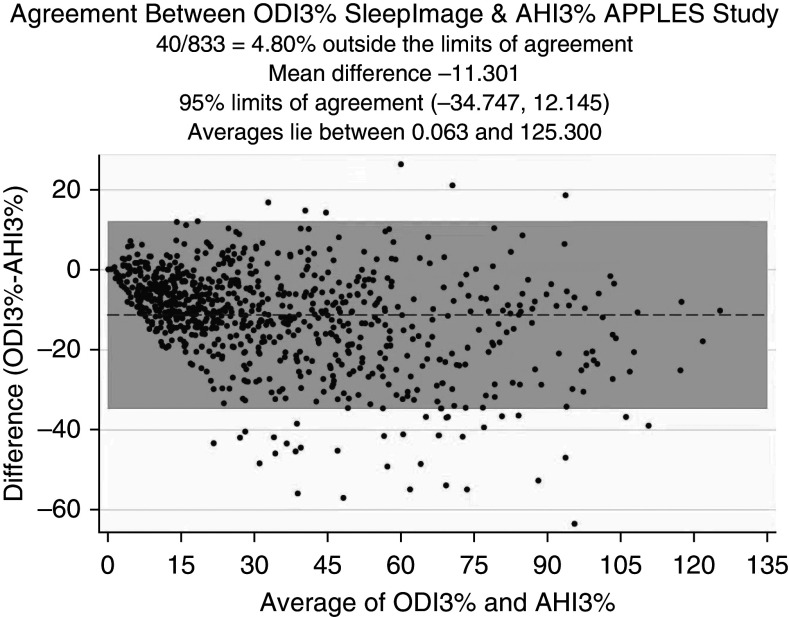
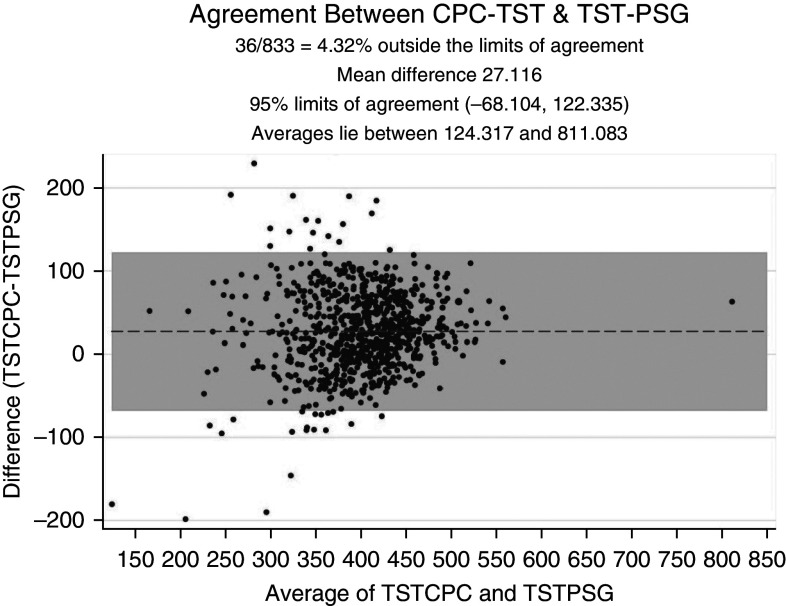
Rationale: The increased prevalence of obstructive sleep apnea (OSA) coincides with a severe shortage of sleep physicians. There is a need for widescale home-sleep-testing devices with accurate automated scoring to accelerate access to treatment.Objectives: To examine the accuracy of an automated apnea-index (AHI) derived from spectral analysis of cardiopulmonary coupling (CPC) extracted from electrocardiograms, combined with oximetry signals, in relation to polysomnograms (PSGs).Methods: Electrocardiograms and pulse-oximeter tracings on PSGs from APPLES (Apnea Positive Pressure Long-term Efficacy Study) were analyzed. Distinct CPC spectral bands were combined with the oxygen desaturation index to create a derived AHI (DAHI). Correlation statistics between the DAHI and the conventionally scored AHI, in which hypopneas required ≥50% airflow reduction alone or a lesser airflow reduction associated with ≥3% desaturation or arousal, using PSGs from APPLES were calculated.Results: A total of 833 adult subjects were included. The DAHI has excellent and strong correlation with the conventionally scored AHI on PSGs, with Pearson coefficients of 0.972 and receiver operating characteristic curves demonstrating strong agreement in all OSA categories: 98.5% in mild OSA (95% confidence interval [CI], 97.6-99.3%), 96.4% in moderate OSA (95% CI, 95.3-97.5%), and 98.5% in severe OSA (95% CI, 97.8-99.2%).Conclusions: An accurate automated AHI can be derived from oximetry and CPC.
Keywords: diagnostic equipment; medical informatics applications; obstructive sleep apnea; pattern recognition.
Figures
References
-
- Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev . 2017;34:70–81. - PubMed
-
- McNicholas WT, Bonsigore MRManagement Committee of EU COST ACTION B26 Sleep apnoea as an independent risk factor for cardiovascular disease: current evidence, basic mechanisms and research priorities Eur Respir J 200729156–178.[Published erratum appears in Eur Respir J 29:614.] - PubMed
-
- Lévy P, Bonsignore MR, Eckel J. Sleep, sleep-disordered breathing and metabolic consequences. Eur Respir J . 2009;34:243–260. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
