

Atypical parathyroid adenoma: clinical and anatomical pathologic features
- PMID: 33472651
- PMCID: PMC7818751
- DOI: 10.1186/s12957-021-02123-7
Atypical parathyroid adenoma: clinical and anatomical pathologic features
Abstract
Background: Primary hyperparathyroidism is an endocrine pathology that affects calcium metabolism. Patients with primary hyperparathyroidism have high concentrations of serum calcium or high concentrations of parathyroid hormone, or incorrect parathyroid hormone levels for serum calcium values. Primary hyperparathyroidism is due to the presence of an adenoma/single-gland disease in 80-85%. Multiple gland disease or hyperplasia accounts for 10-15% of cases of primary hyperparathyroidism. Atypical parathyroid adenoma and parathyroid carcinoma are both responsible for about 1.2-1.3% and 1% or less of primary hyperparathyroidism, respectively.
Methods: We performed a retrospective cohort study and enrolled 117 patients with primary hyperparathyroidism undergoing minimally invasive parathyroidectomy. Histological and immunohistochemical examination showed that 107 patients (91.5%) were diagnosed with typical adenoma (group A), while 10 patients (8.5%) were diagnosed with atypical parathyroid adenoma (group B). None of the patients were affected by parathyroid carcinoma.
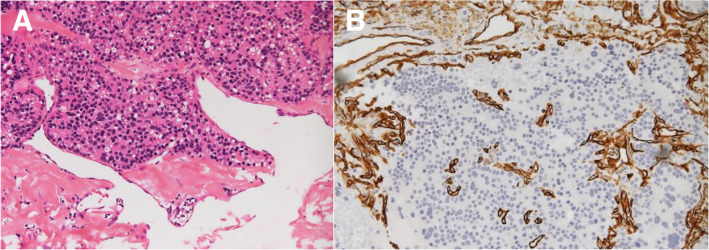
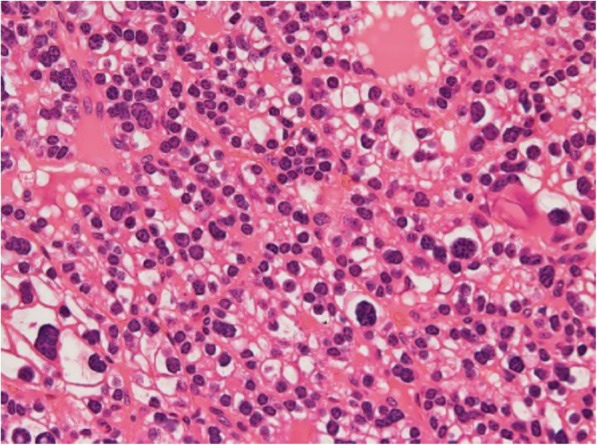
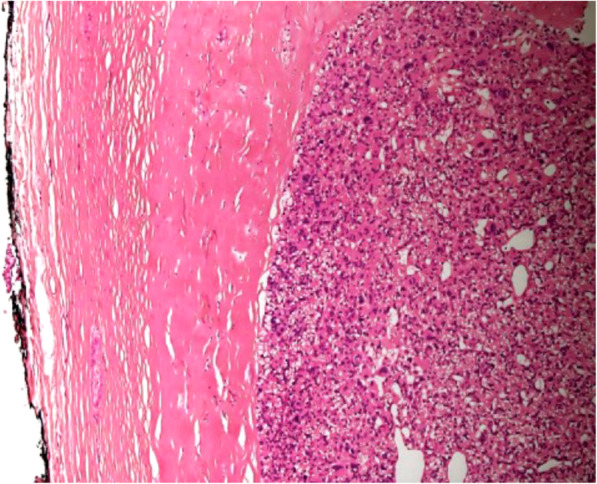
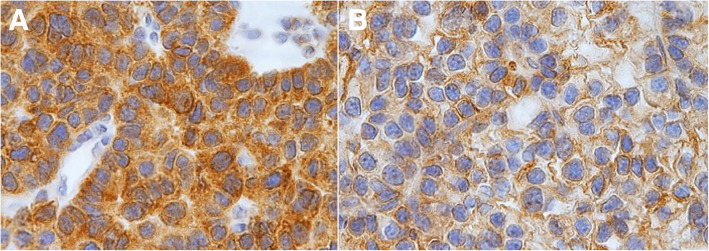
Results: Significant statistical differences were found in histological and immunohistochemical parameters as pseudocapsular invasion (p < 0.001), bands of fibrosis (p < 0.001), pronounced trabecular growth (p < 0.001), mitotic rates of > 1/10 high-power fields (HPFs) (p < 0.001), nuclear pleomorphism (p = 0.036), thick capsule (p < 0.001), Ki-67+ > 4% (p < 0.001), galectin-3 + (p = 0.002), and protein gene product (PGP) 9.5 + (p = 0.038).
Conclusions: Atypical parathyroid adenoma is a tumor that has characteristics both of typical adenoma and parathyroid carcinoma. The diagnosis is reached by excluding with strict methods the presence of malignancy criteria. Atypical parathyroid adenoma compared to typical adenoma showed significant clinical, hematochemical, histological, and immunohistochemical differences. We did not find any disease relapse in the 10 patients with atypical parathyroid adenoma during 60 months of follow-up time.
Keywords: Atypical parathyroid adenoma; Minimally invasive parathyroidectomy; Parathyroid carcinoma; Primary hyperparathyroidism; Typical adenoma.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
