

Advanced echocardiographic phenotyping of critically ill patients with coronavirus-19 sepsis: a prospective cohort study
- PMID: 33472693
- PMCID: PMC7816136
- DOI: 10.1186/s40560-020-00516-6
Advanced echocardiographic phenotyping of critically ill patients with coronavirus-19 sepsis: a prospective cohort study
Abstract
Background: Sepsis is characterized by various hemodynamic alterations which could happen concomitantly in the heart, pulmonary and systemic circulations. A comprehensive demonstration of their interactions in the clinical setting of COVID-19 sepsis is lacking. This study aimed at evaluating the feasibility, clinical implications, and physiological coherence of the various indices of hemodynamic function and acute myocardial injury (AMI) in COVID-19 sepsis.
Methods: Hemodynamic and echocardiographic data of septic critically ill COVID-19 patients were prospectively recorded. A dozen hemodynamic indices exploring contractility and loading conditions were assessed. Several cardiac biomarkers were measured, and AMI was considered if serum concentration of high-sensitive troponin T (hs-TNT) was above the 99th percentile, upper reference.
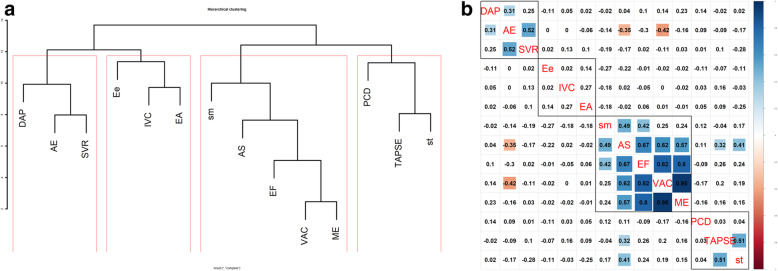
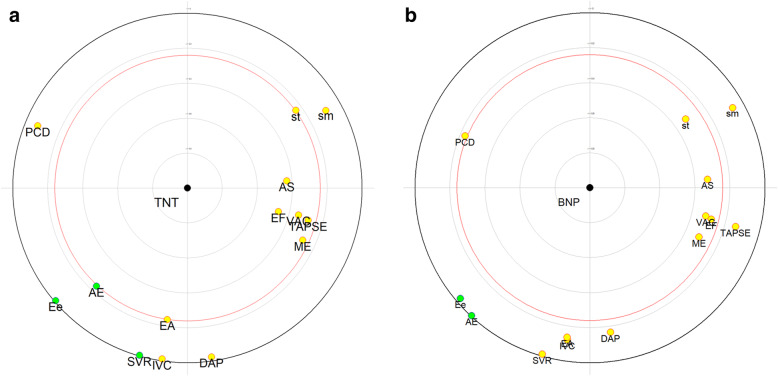
Results: Sixty-seven patients were assessed (55 males), with a median age of 61 [50-70] years. Overall, the feasibility of echocardiographic parameters was very good, ranging from 93 to 100%. Hierarchical clustering method identified four coherent clusters involving cardiac preload, left ventricle (LV) contractility, LV afterload, and right ventricle (RV) function. LV contractility indices were not associated with preload indices, but some of them were positively correlated with RV function parameters and negatively correlated with a single LV afterload parameter. In most cases (n = 36, 54%), echocardiography results prompted therapeutic changes. Mortality was not influenced by the echocardiographic variables in multivariable analysis. Cardiac biomarkers' concentrations were most often increased with high incidence of AMI reaching 72%. hs-TNT was associated with mortality and inversely correlated with most of LV and RV contractility indices.
Conclusions: In this comprehensive hemodynamic evaluation in critically ill COVID-19 septic patients, we identified four homogeneous and coherent clusters with a good feasibility. AMI was common and associated with alteration of LV and RV functions. Echocardiographic assessment had a clinical impact on patient management in most cases.
Keywords: Afterload; COVID-19; Cardiac dysfunction; Sepsis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
