

Recalcitrant infective scleritis masquerading an autoimmune necrotising scleritis: a primary presentation of biopsy-proven granulomatosis with polyangiitis
- PMID: 33472807
- PMCID: PMC10577764
- DOI: 10.1136/bcr-2020-239517
Recalcitrant infective scleritis masquerading an autoimmune necrotising scleritis: a primary presentation of biopsy-proven granulomatosis with polyangiitis
Abstract
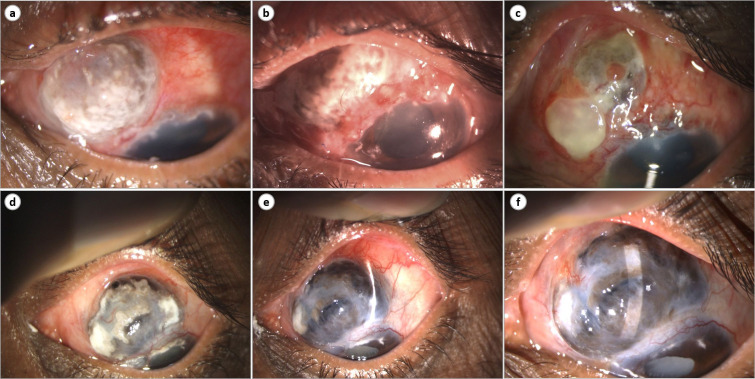
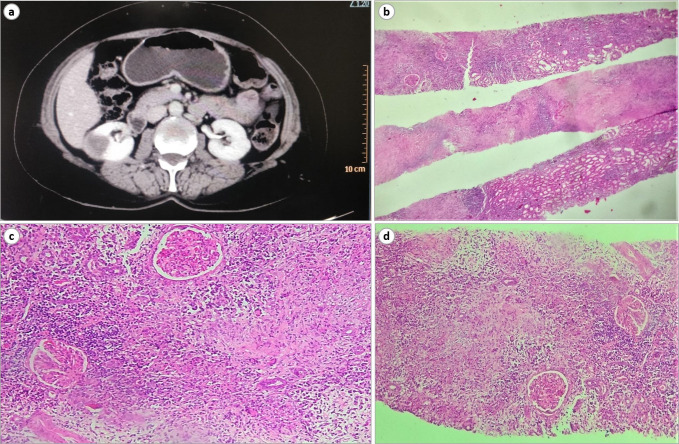
Infectious scleritis is a rare but important cause of scleral inflammation. It is usually associated with an underlying ocular (prior ocular surgery or trauma) or systemic risk factor. A 53-year-old apparently systemically healthy woman presenting with spontaneous-onset pain, redness and watering in the left eye for 10 days was diagnosed with culture-proven Pseudomonas aeruginosa anterior scleritis. However, she was non-responsive to organism-sensitive antibiotics and scleral graft was performed twice, which showed graft re-infection. On repeated extensive systemic evaluations, the patient was diagnosed with biopsy-proven granulomatosis with polyangiitis (GPA). The patient was started on mycophenolate mofetil for both induction and maintenance phases and showed dramatic improvement with no recurrence till 1 year follow-up. High index of suspicion for autoimmune disorders, especially GPA, must be maintained for unilateral relentless infective scleritis masquerading as autoimmune necrotising scleritis. Mycophenolate mofetil holds a promising role for inducing as well as maintaining disease remission in ocular GPA.
Keywords: anterior chamber; ophthalmology.
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Scleritis in patients with granulomatosis with polyangiitis (Wegener).Br J Ophthalmol. 2016 Aug;100(8):1062-5. doi: 10.1136/bjophthalmol-2015-307460. Epub 2015 Nov 13. Br J Ophthalmol. 2016. PMID: 26567022
-
Rituximab therapy combined with methotrexate for severe necrotizing scleritis in a case of granulomatosis with polyangiitis.Indian J Ophthalmol. 2020 Sep;68(9):1981-1983. doi: 10.4103/ijo.IJO_2249_19. Indian J Ophthalmol. 2020. PMID: 32823449 Free PMC article.
-
Clinical profile and management of granulomatosis with polyangiitis-associated scleritis from a tertiary care hospital in South India.Indian J Ophthalmol. 2023 Jan;71(1):146-152. doi: 10.4103/ijo.IJO_1411_22. Indian J Ophthalmol. 2023. PMID: 36588225 Free PMC article.
-
Necrotizing Scleritis: A Review.Ocul Immunol Inflamm. 2024 Sep;32(7):1405-1419. doi: 10.1080/09273948.2023.2206898. Epub 2023 Jun 6. Ocul Immunol Inflamm. 2024. PMID: 37279404 Review.
-
Updates of ocular involvement in granulomatosis with polyangiitis.Graefes Arch Clin Exp Ophthalmol. 2023 Jun;261(6):1515-1523. doi: 10.1007/s00417-022-05918-w. Epub 2022 Dec 7. Graefes Arch Clin Exp Ophthalmol. 2023. PMID: 36473987 Review.
Cited by
-
Infectious Scleritis Masquerading as Isolated Orbital Cellulitis: A Case Report.Cureus. 2025 Jun 10;17(6):e85714. doi: 10.7759/cureus.85714. eCollection 2025 Jun. Cureus. 2025. PMID: 40642687 Free PMC article.
-
Infectious scleritis: a review of etiologies, clinical features, and management strategies.Front Ophthalmol (Lausanne). 2025 Feb 7;5:1493831. doi: 10.3389/fopht.2025.1493831. eCollection 2025. Front Ophthalmol (Lausanne). 2025. PMID: 39990248 Free PMC article. Review.
References
-
- Biswas J, Babu K, Gopal L, et al. . Ocular manifestations of Wegener's granulomatosis. Analysis of nine cases. Indian J Ophthalmol 2003;51:217. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical