

Phase I Trial of DNA Methyltransferase Inhibitor Guadecitabine Combined with Cisplatin and Gemcitabine for Solid Malignancies Including Urothelial Carcinoma (SPIRE)
- PMID: 33472913
- PMCID: PMC7611191
- DOI: 10.1158/1078-0432.CCR-20-3946
Phase I Trial of DNA Methyltransferase Inhibitor Guadecitabine Combined with Cisplatin and Gemcitabine for Solid Malignancies Including Urothelial Carcinoma (SPIRE)
Abstract
Purpose: Preclinical data indicate that DNA methyltransferase inhibition will circumvent cisplatin resistance in various cancers.
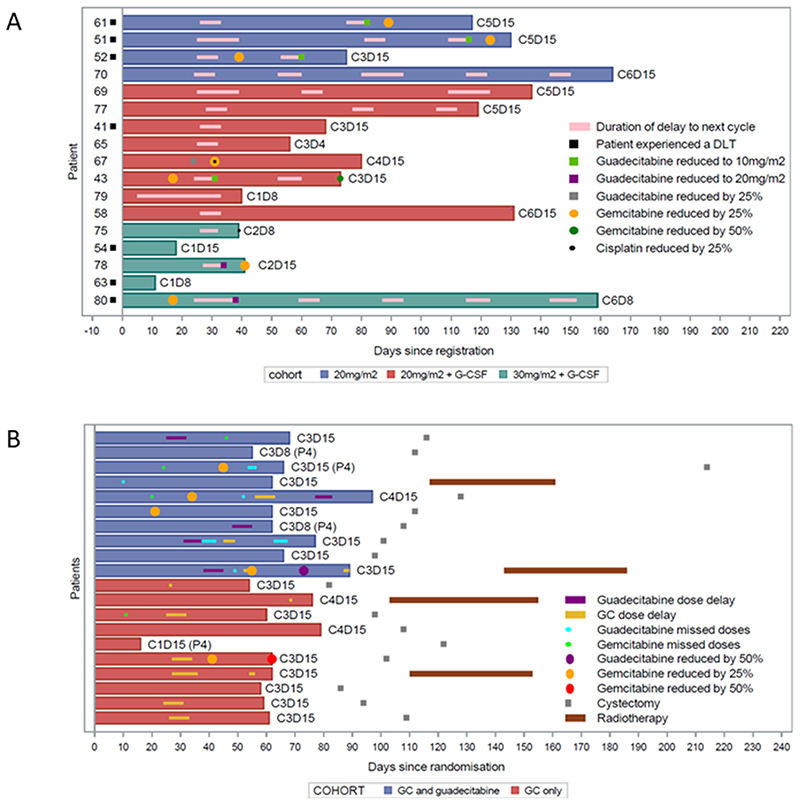
Patient and methods: SPIRE comprised a dose-escalation phase for incurable metastatic solid cancers, followed by a randomized dose expansion phase for neoadjuvant treatment of T2-4a N0 M0 bladder urothelial carcinoma. The primary objective was a recommended phase II dose (RP2D) for guadecitabine combined with gemcitabine and cisplatin. Treatment comprised 21-day gemcitabine and cisplatin cycles (cisplatin 70 mg/m2, i.v., day 8 and gemcitabine 1,000 mg/m2, i.v., days 8 + 15). Guadecitabine was injected subcutaneously on days 1-5, within escalation phase cohorts, and to half of 20 patients in the expansion phase. Registration ID: ISRCTN 16332228.
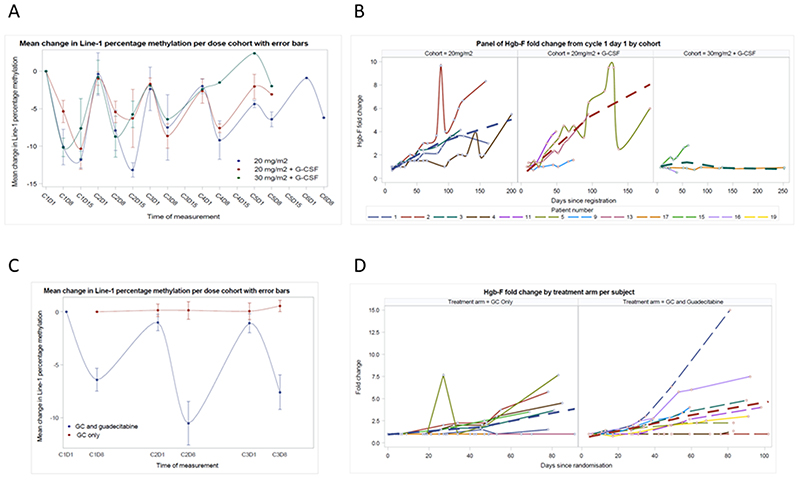
Results: Within the escalation phase, dose-limiting toxicities related predominantly to myelosuppression requiring G-CSF prophylaxis from cohort 2 (guadecitabine 20 mg/m2, days 1-5). The most common grade ≥3 adverse events in 17 patients in the dose-escalation phase were neutropenia (76.5%), thrombocytopenia (64.7%), leukopenia (29.4%), and anemia (29.4%). Addition of guadecitabine to gemcitabine and cisplatin in the expansion phase resulted in similar rates of severe hematologic adverse events, similar cisplatin dose intensity, but modestly reduced gemcitabine dose intensity. Radical treatment options after chemotherapy were not compromised. Pharmacodynamics evaluations indicated guadecitabine maximal target effect at the point of cisplatin administration. Pharmacokinetics were consistent with prior data. No treatment-related deaths occurred.
Conclusions: The guadecitabine RP2D was 20 mg/m2, days 1-5, in combination with gemcitabine and cisplatin and required GCSF prophylaxis. Gene promoter methylation pharmacodynamics are optimal with this schedule. Addition of guadecitabine to gemcitabine and cisplatin was tolerable, despite some additional myelosuppression, and warrants further investigation to assess efficacy.
©2021 American Association for Cancer Research.
Conflict of interest statement
SJC reports consulting or advisory roles for Roche, Janssen Cilag, MSD, Astellas, Bayer and AstraZeneca, and research funding provision from Astex Pharmaceuticals, AstraZenaca and Clovis Oncology. SD reports consultancy or advisory roles for GSK, Incanthera and Boehringer Ingelheim, and research funding from Amgen. JWFC has received reimbursement for consultancy from Astra Zeneca, Roche and Janssen, speaker fees from BMS, MSD, Nucleix and Roche, and honoraria for membership of an advisory board for Ferring. NS has received speaker fees from Pfizer, EUSA Pharma and BMS. DE has received speaker fees from AstraZeneca, Pfizer, Janssen and MSD. RAH has received honoraria related membership from advisory boards from MSD, Roche, Nektar pharmaceuticals, Janssen, BMS Bayer and Astellas and speakers fees from Roche and Janssen. DC is employed by Astex Pharmaceuticals, Inc. All remaining authors have declared no conflicts of interest.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
-
- International collaboration of trialists on behalf of the Medical Research Council Advanced Bladder Cancer Working Party, EORTC Genito-Urinary Group ABCSG, Group NCIoCCT, Finnbladder NBCSG, group CUEdTOC. Neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive bladder cancer: a randomised controlled trial. International collaboration of trialists. Lancet. 1999;354(9178):533–40. - PubMed
-
- von der Maase H, Hansen SW, Roberts JT, Dogliotti L, Oliver T, Moore MJ, et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: results of a large, randomized, multinational, multicenter, phase III study. J Clin Oncol. 2000;18(17):3068–77. - PubMed
-
- Crabb SJ, Douglas J. The latest treatment options for bladder cancer. Br Med Bull. 2018;128(1):85–95. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
