

Incidence, Prevalence, and Geographical Clustering of Motor Neuron Disease in the Netherlands
- PMID: 33472922
- PMCID: PMC8055340
- DOI: 10.1212/WNL.0000000000011467
Incidence, Prevalence, and Geographical Clustering of Motor Neuron Disease in the Netherlands
Abstract
Objective: To assess time trends in motor neuron disease (MND) incidence, prevalence, and mortality and to investigate geographic clustering of MND cases in the Netherlands from 1998 to 2017, we analyzed data from the Netherlands Personal Records database, the Netherlands MND Center, and the Netherlands Patient Association of Neuromuscular Diseases.
Methods: In this prospective cohort study, Poisson regression was used to assess time trends in MND risk. We calculated age- and sex-standardized, observed, and expected cases for 1,694 areas. Bayesian smoothed risk mapping was used to investigate geographic MND risk.
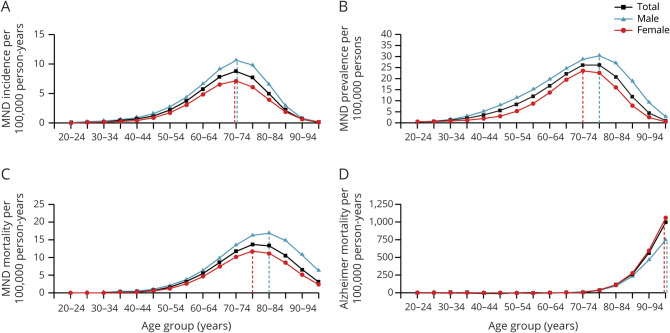
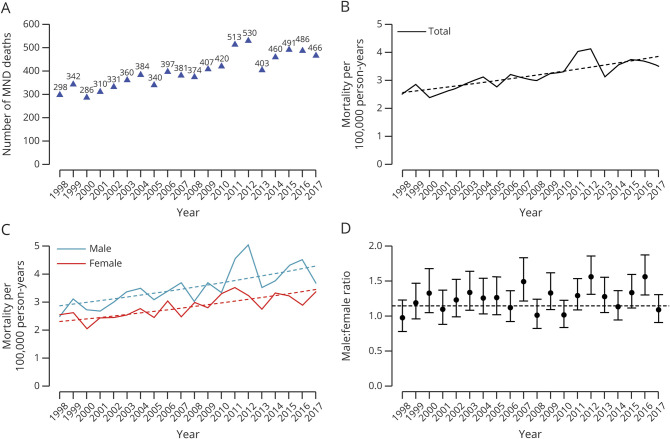
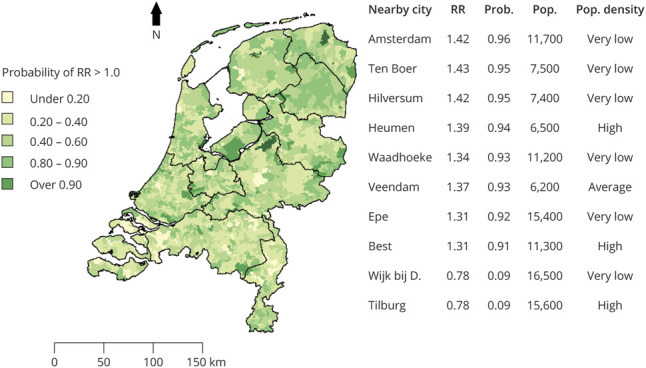
Results: We identified 7,992 MND cases, reflecting an incidence of 2.64 (95% confidence interval [CI] 2.62-2.67) per 100,000 person-years and a prevalence of 9.5 (95% CI 9.1-10.0) per 100,000 persons. Highest age-standardized prevalence and mortality rates occurred at a later age in men than in women (p < 0.001). Unadjusted mortality rates increased by 53.2% from 2.57 per 100,000 person-years in 1998 to 3.86 per 100,000 person-years in 2017. After adjustment for age and sex, an increase in MND mortality rate of 14.1% (95% CI 5.7%-23.2%, p < 0.001) remained. MND relative risk ranged from 0.78 to 1.43 between geographic areas; multiple urban and rural high-risk areas were identified.
Conclusions: We found a significant national increase in MND mortality from 1998 through 2017, explained only partly by an aging Dutch population, and a geographic variability in MND risk, suggesting a role for environmental or demographic risk factors.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources