

Imaging coronary plaques using 3D motion-compensated [18F]NaF PET/MR
- PMID: 33474584
- PMCID: PMC8241750
- DOI: 10.1007/s00259-020-05180-4
Imaging coronary plaques using 3D motion-compensated [18F]NaF PET/MR
Abstract
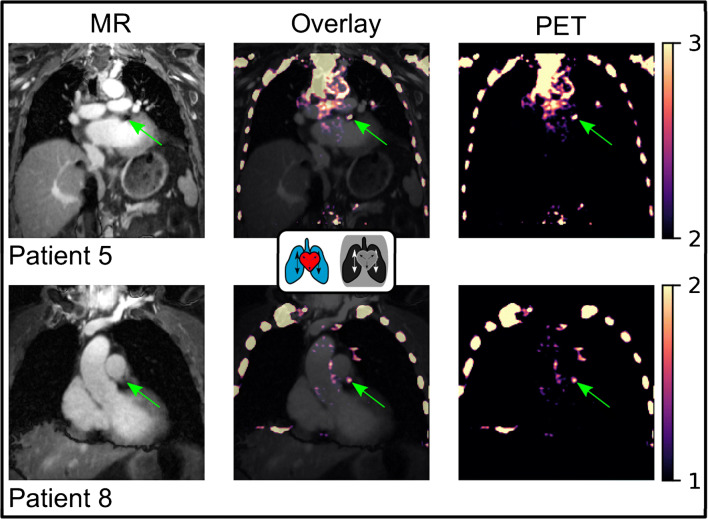
Background: Cardiac PET has recently found novel applications in coronary atherosclerosis imaging using [18F]NaF as a radiotracer, highlighting vulnerable plaques. However, the resulting uptakes are relatively small, and cardiac motion and respiration-induced movement of the heart can impair the reconstructed images due to motion blurring and attenuation correction mismatches. This study aimed to apply an MR-based motion compensation framework to [18F]NaF data yielding high-resolution motion-compensated PET and MR images.
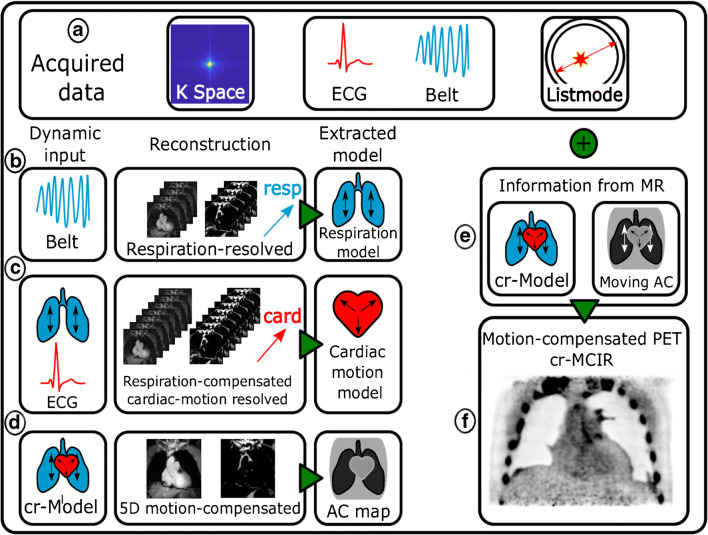
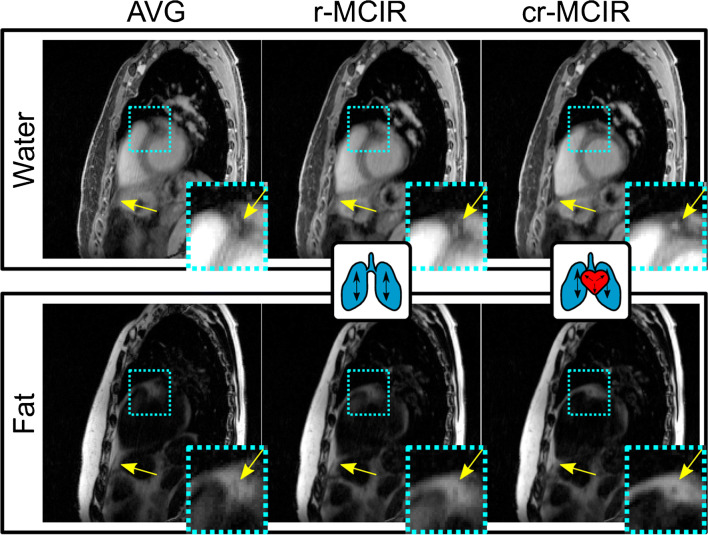
Methods: Free-breathing 3-dimensional Dixon MR data were acquired, retrospectively binned into multiple respiratory and cardiac motion states, and split into fat and water fraction using a model-based reconstruction framework. From the dynamic MR reconstructions, both a non-rigid cardiorespiratory motion model and a motion-resolved attenuation map were generated and applied to the PET data to improve image quality. The approach was tested in 10 patients and focal tracer hotspots were evaluated concerning their target-to-background ratio, contrast-to-background ratio, and their diameter.
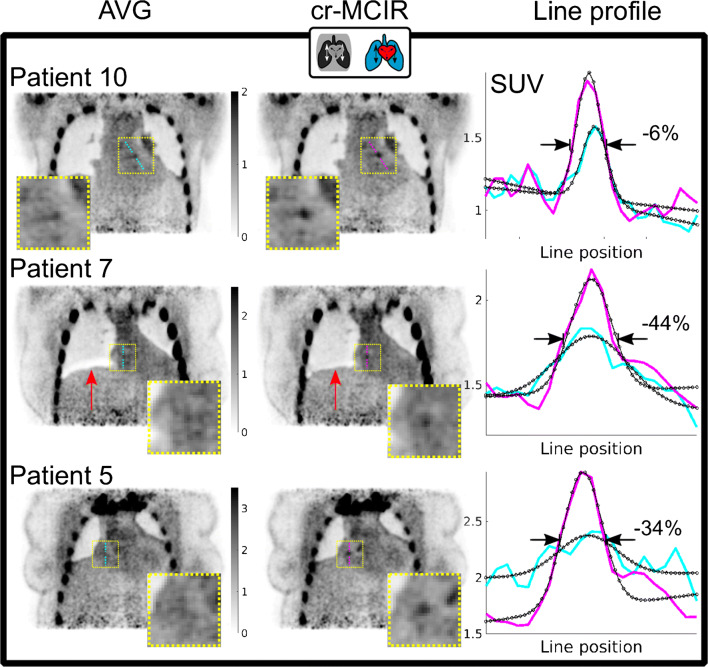
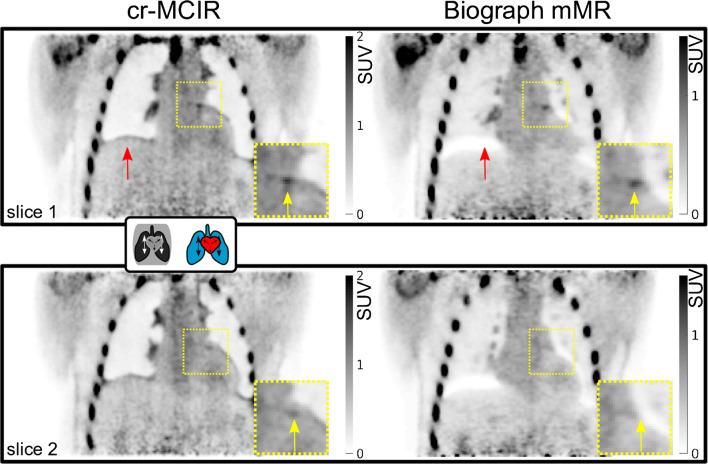
Results: MR-based motion models were successfully applied to compensate for physiological motion in both PET and MR. Target-to-background ratios of identified plaques improved by 7 ± 7%, contrast-to-background ratios by 26 ± 38%, and the plaque diameter decreased by -22 ± 18%. MR-based dynamic attenuation correction strongly reduced attenuation correction artefacts and was not affected by stent-related signal voids in the underlying MR reconstructions.
Conclusions: The MR-based motion correction framework presented here can improve the target-to-background, contrast-to-background, and width of focal tracer hotspots in the coronary system. The dynamic attenuation correction could effectively mitigate the risk of attenuation correction artefacts in the coronaries at the lung-soft tissue boundary. In combination, this could enable a more reproducible and reliable plaque localisation.
Keywords: Atherosclerosis,; Cardiac and respiratory motion; Motion compensation,; Simultaneous PET/MR,; [18F]NaF cardiac imaging,.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
