

Development and Validation of a Simplified Probability Assessment Score Integrated With Age-Adjusted d-Dimer for Diagnosis of Acute Aortic Syndromes
- PMID: 33474974
- PMCID: PMC7955418
- DOI: 10.1161/JAHA.120.018425
Development and Validation of a Simplified Probability Assessment Score Integrated With Age-Adjusted d-Dimer for Diagnosis of Acute Aortic Syndromes
Abstract
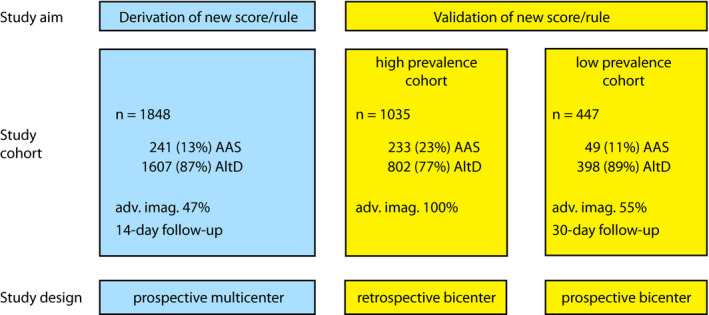
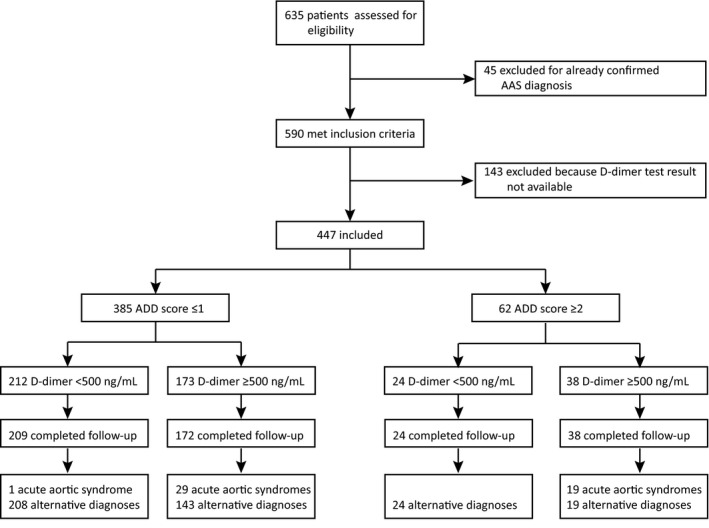
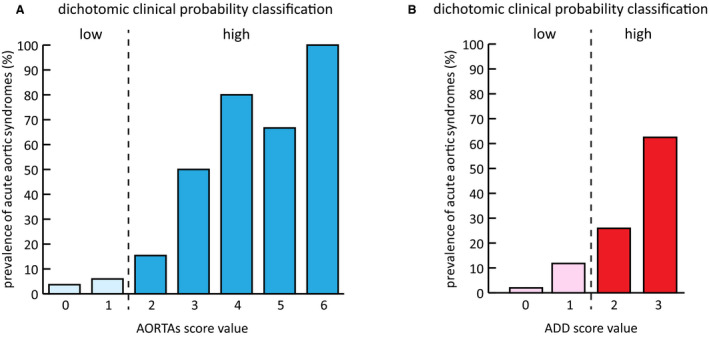
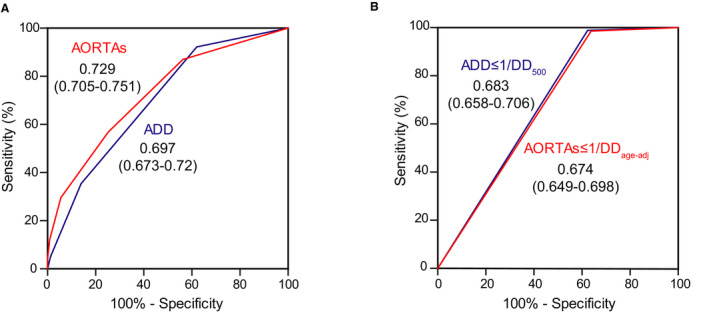
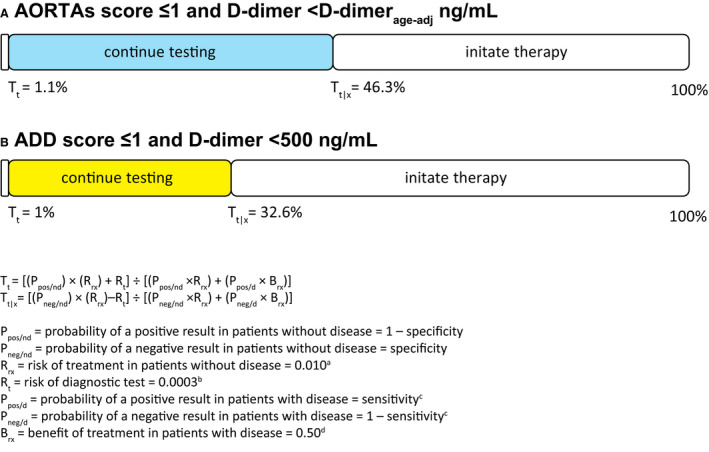
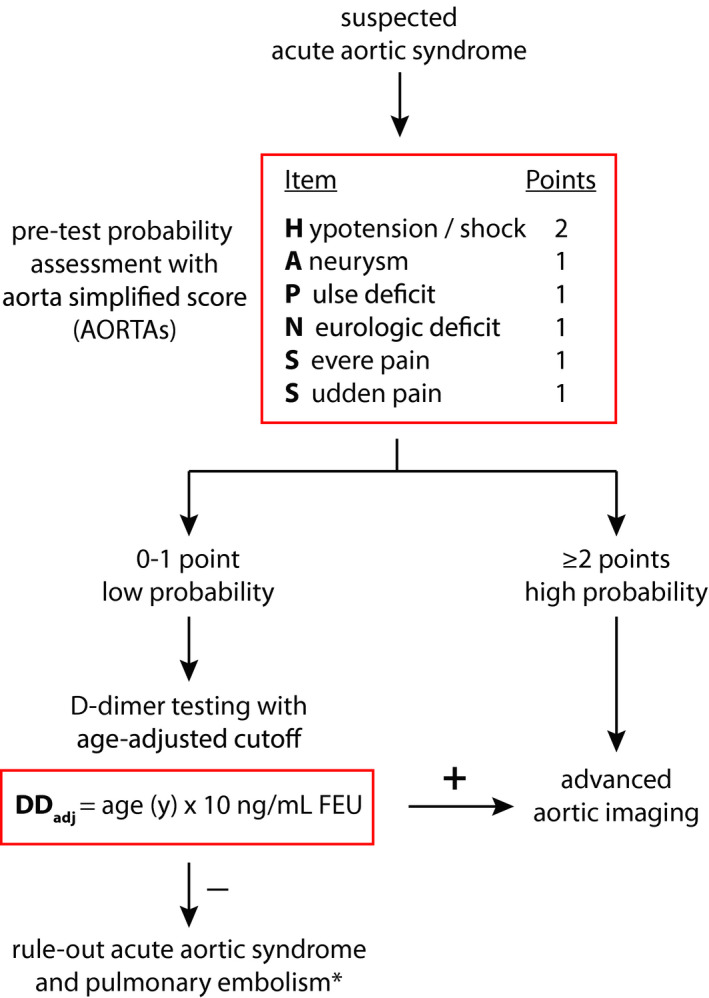
Background When acute aortic syndromes (AASs) are suspected, pretest clinical probability assessment and d-dimer (DD) testing are diagnostic options allowing standardized care. Guidelines suggest use of a 12-item/3-category score (aortic dissection detection) and a DD cutoff of 500 ng/mL. However, a simplified assessment tool and a more specific DD cutoff could be advantageous. Methods and Results In a prospective derivation cohort (n=1848), 6 items identified by logistic regression (thoracic aortic aneurysm, severe pain, sudden pain, pulse deficit, neurologic deficit, hypotension), composed a simplified score (AORTAs) assigning 2 points to hypotension and 1 to the other items. AORTAs≤1 and ≥2 defined low and high clinical probability, respectively. Age-adjusted DD was calculated as years/age × 10 ng/mL (minimum 500). The AORTAs score and AORTAs≤1/age-adjusted DD rule were validated in 2 patient cohorts: a high-prevalence retrospective cohort (n=1035; 22% AASs) and a low-prevalence prospective cohort (n=447; 11% AASs) subjected to 30-day follow-up. The AUC of the AORTAs score was 0.729 versus 0.697 of the aortic dissection detection score (P=0.005). AORTAs score assessment reclassified 16.6% to 25.1% of patients, with significant net reclassification improvement of 10.3% to 32.7% for AASs and -8.6 to -17% for alternative diagnoses. In both cohorts, AORTAs≥2 had superior sensitivity and slightly lower specificity than aortic dissection detection ≥2. In the prospective validation cohort, AORTAs≤1/age-adjusted DD had a sensitivity of 100%, a specificity of 48.6%, and an efficiency of 43.3%. Conclusions AORTAs is a simplified score with increased sensitivity, improved AAS classification, and minor trade-off in specificity, amenable to integration with age-adjusted DD for diagnostic rule-out.
Keywords: age; aorta; diagnosis; dissection; d‐dimer; syndrome.
Conflict of interest statement
FM reports honoraria from Boehringer Ingelheim and Bayer for lectures and educational activities unrelated to the present work. The remaining authors have no disclosures to report.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
