

Best Practices: Hip Femoroacetabular Impingement
- PMID: 33474984
- PMCID: PMC8116615
- DOI: 10.2214/AJR.20.22783
Best Practices: Hip Femoroacetabular Impingement
Abstract
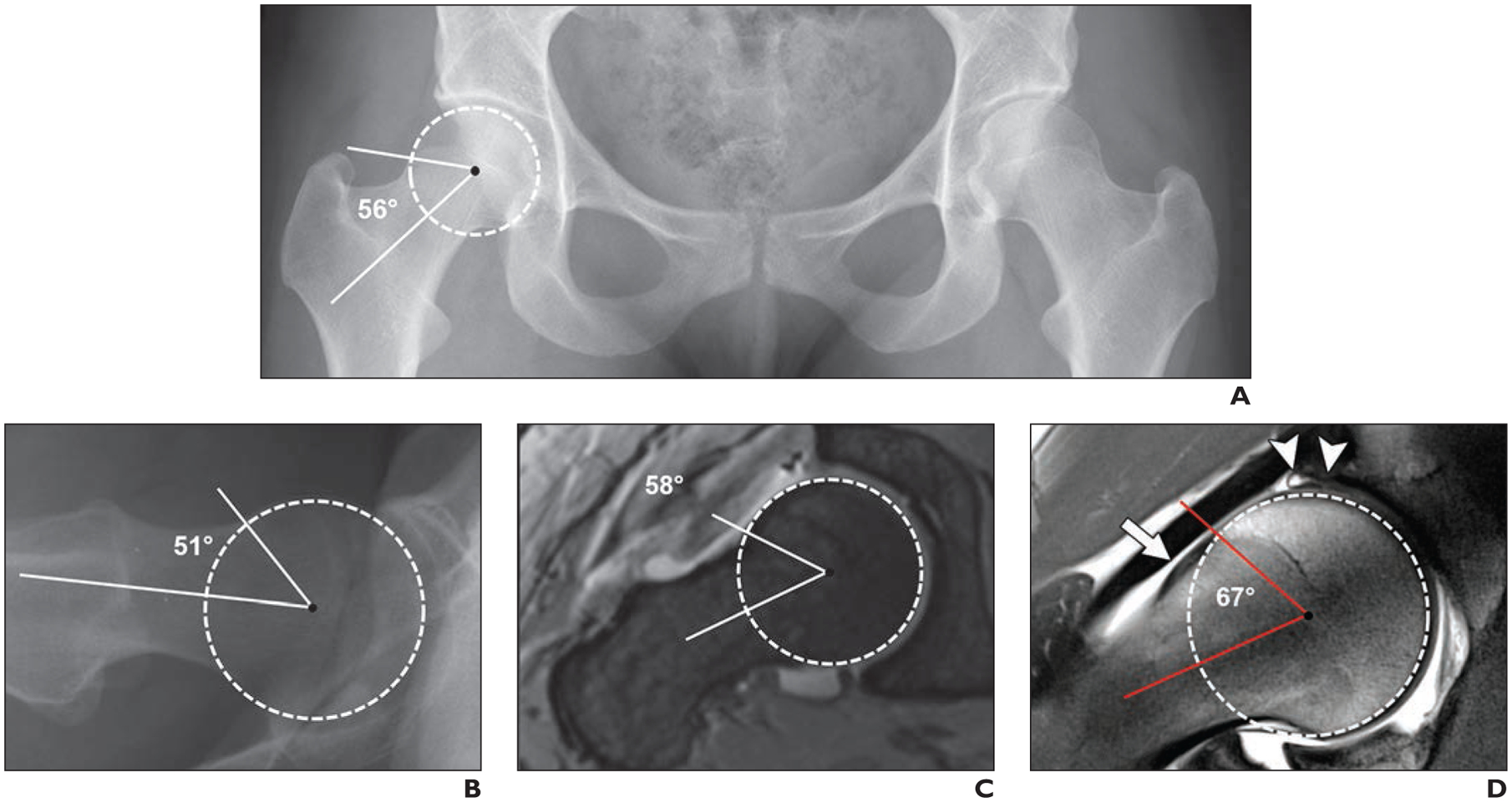
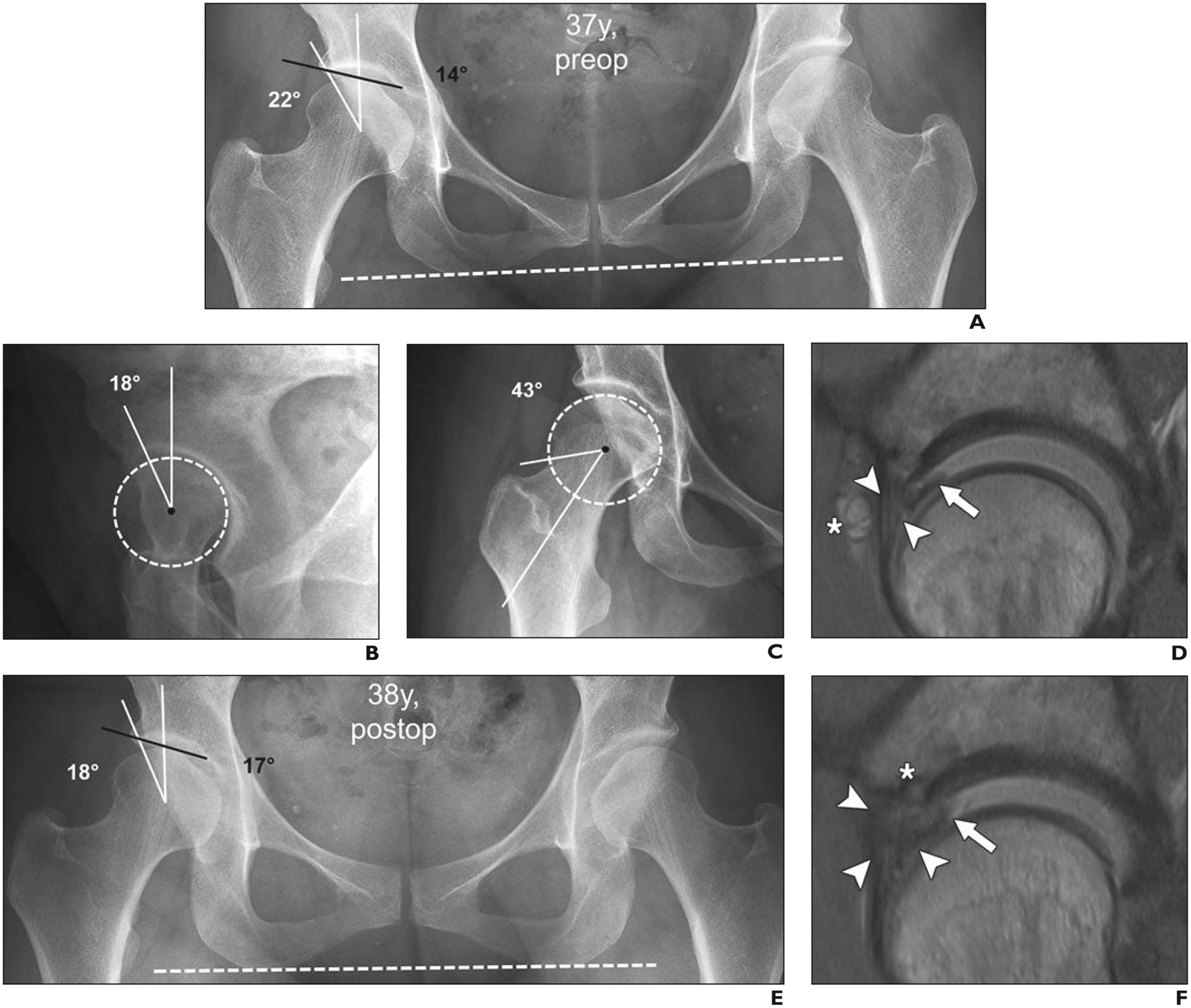
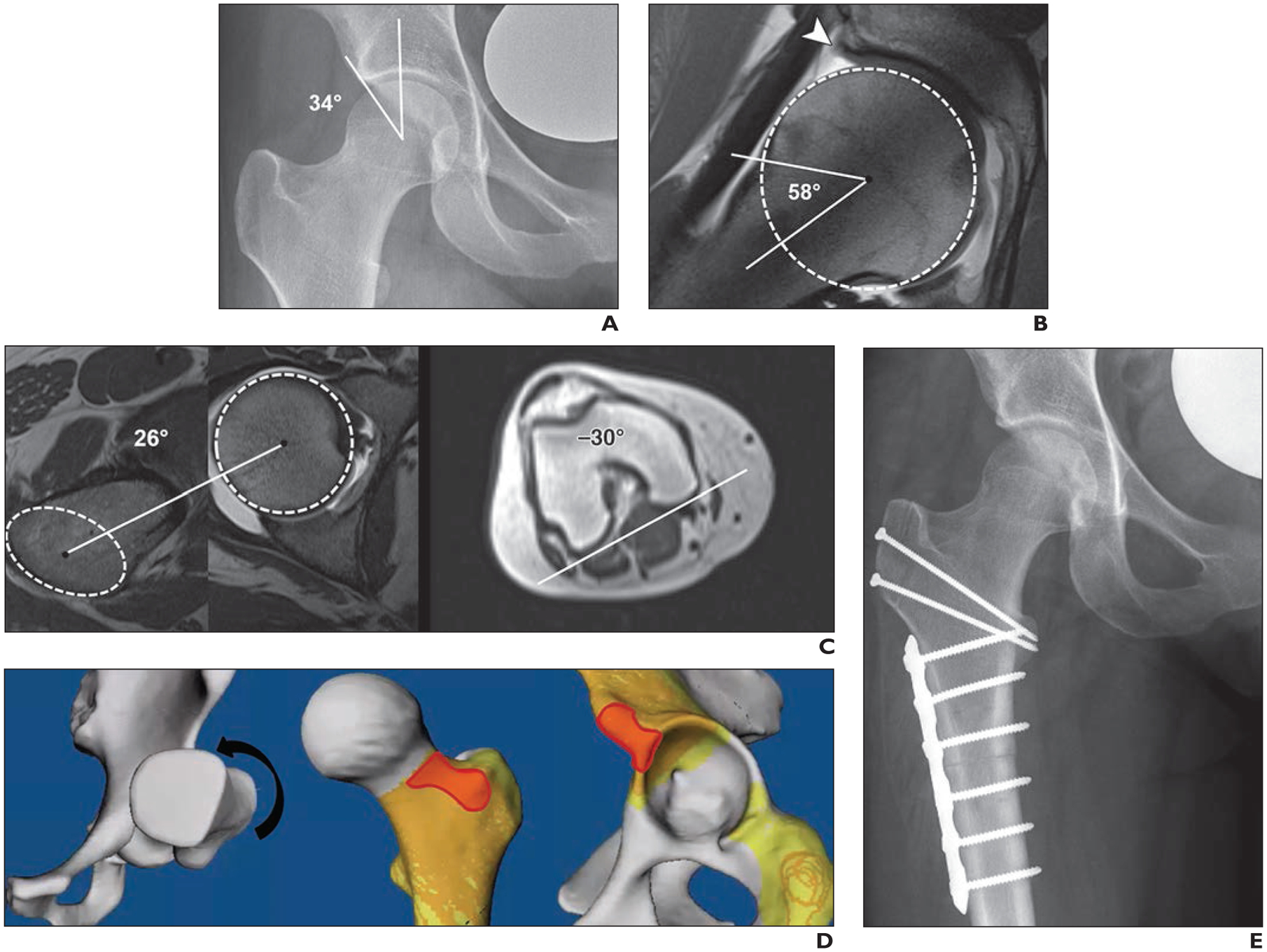
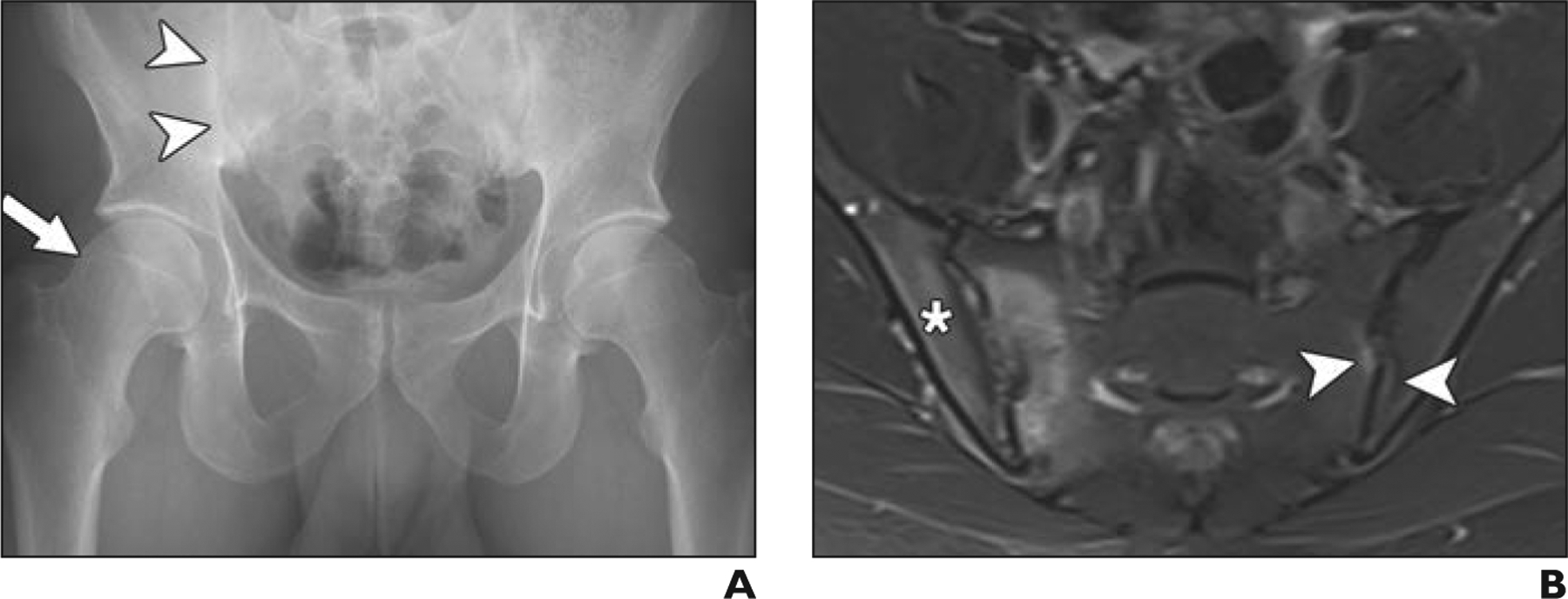
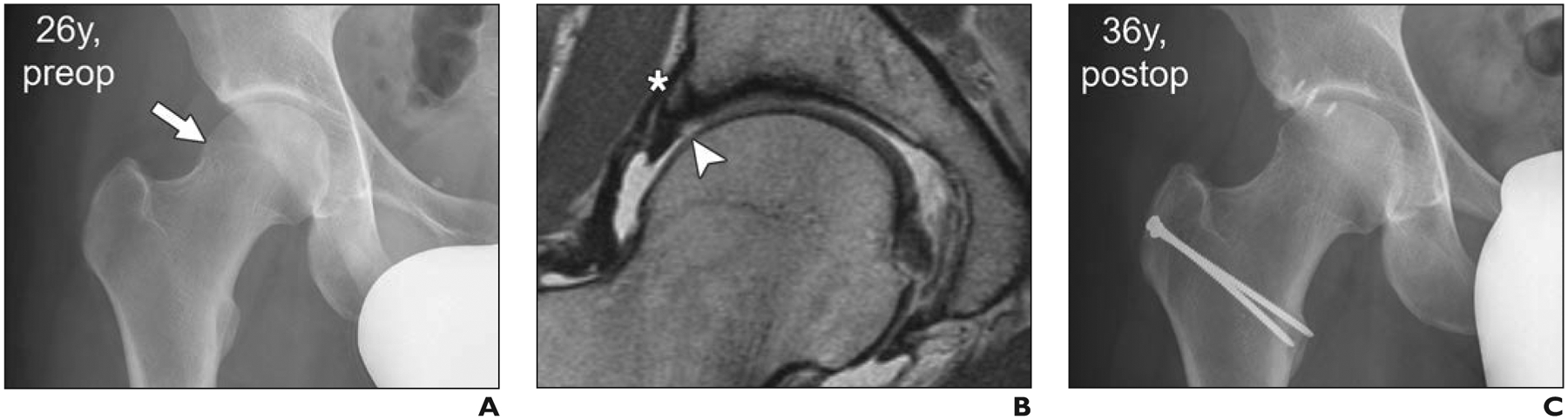
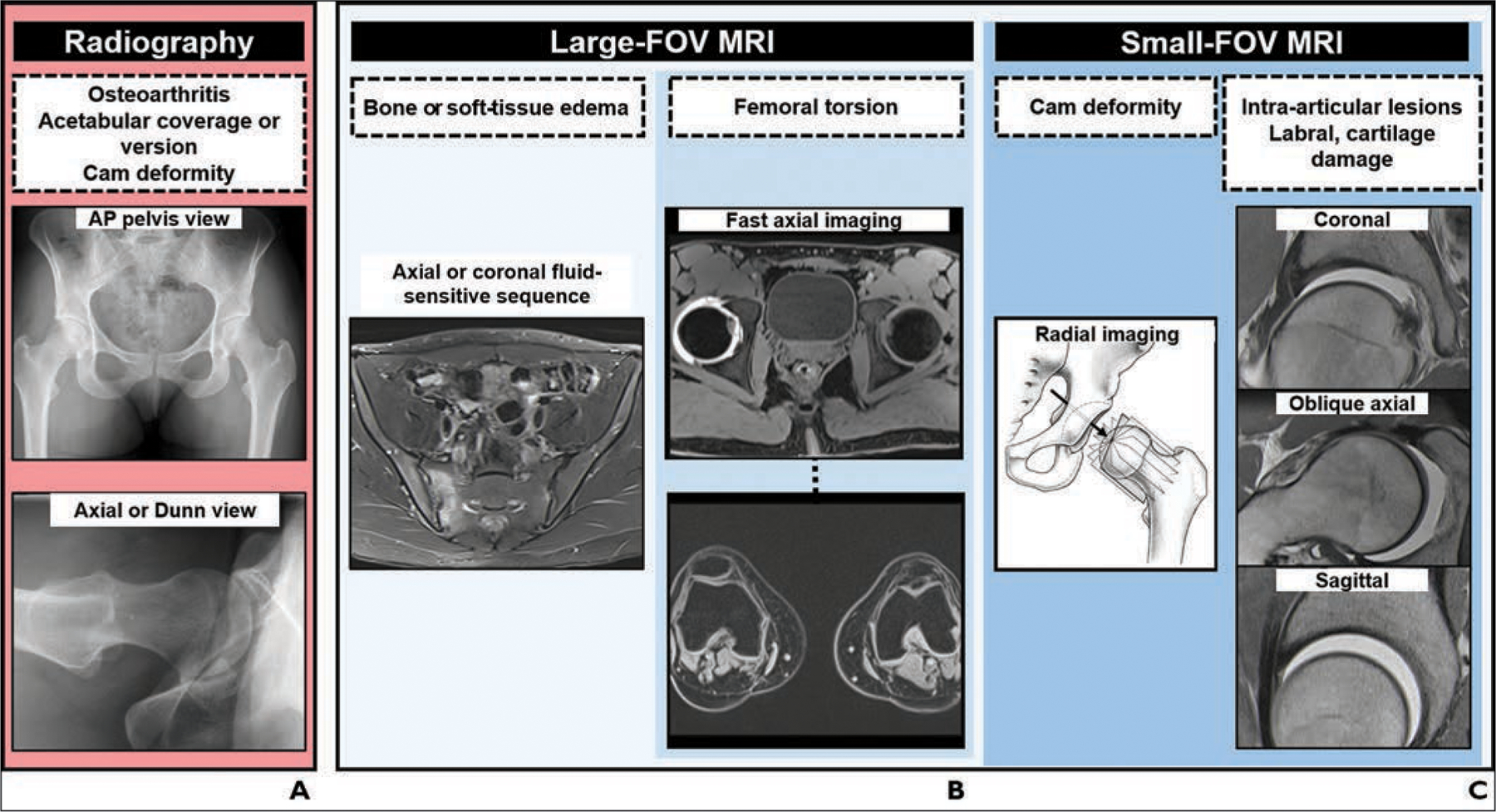
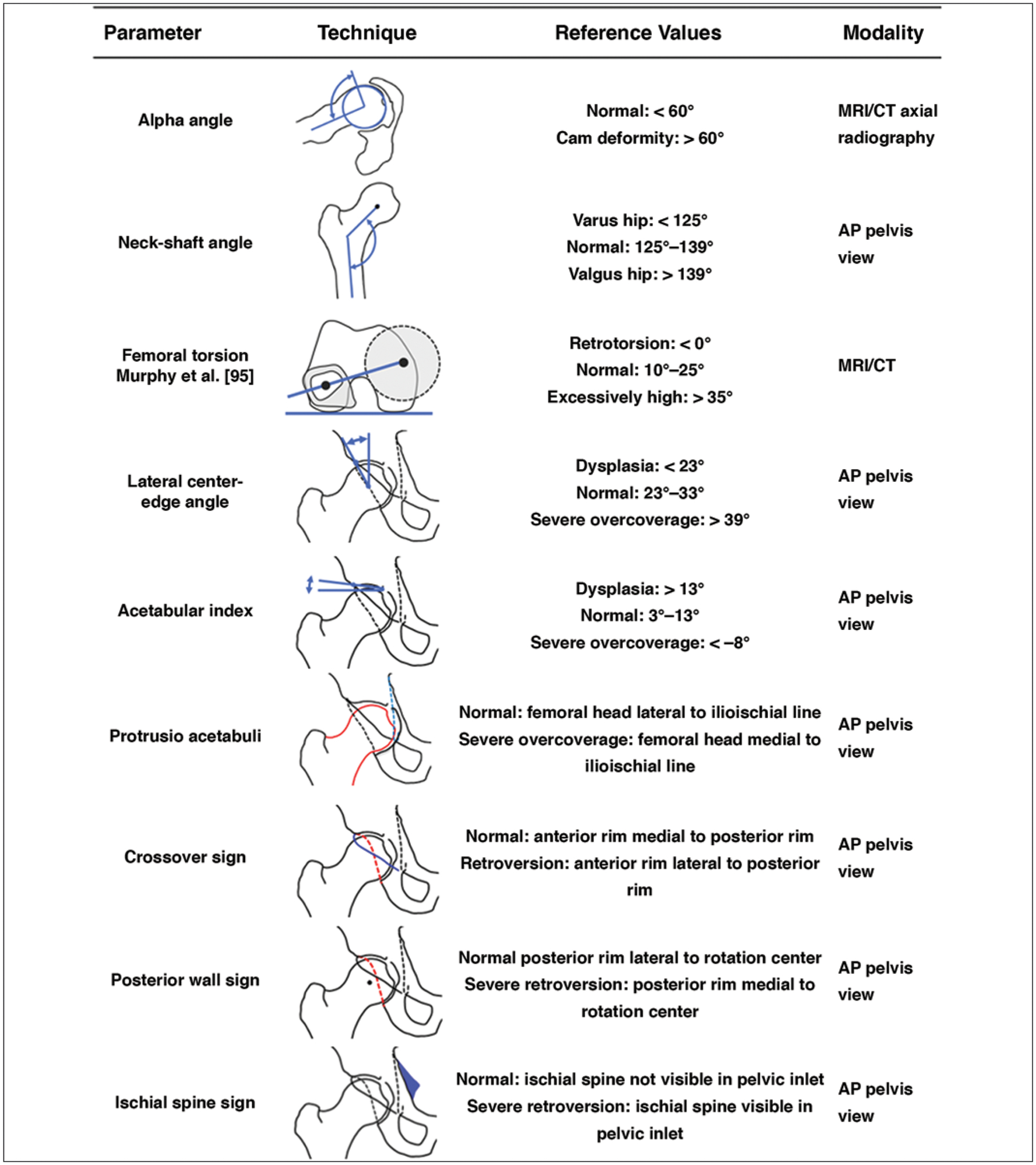
OBJECTIVE. Imaging plays a critical role in the assessment of patients with femoroacetabular impingement (FAI). With better understanding of the underlying pathomechanics and advances in joint-preserving surgery, there is an increasing need to define the most appropriate imaging workup. The purpose of this article is to provide guidance on best practices for imaging of patients with FAI in light of recent advances in corrective FAI surgery. CONCLUSION. Pelvic radiography with dedicated hip projections is the basis of the diagnostic workup of patients with suspected FAI to assess arthritic changes and acetabular coverage and to screen for cam deformities. Chondrolabral lesions should be evaluated with unenhanced MRI or MR arthrography. The protocol should include a large-FOV fluid-sensitive sequence to exclude conditions that can mimic or coexist with FAI, radial imaging to accurately determine the presence of a cam deformity, and imaging of the distal femoral condyles for measurement of femoral torsion. CT remains a valuable tool for planning of complex surgical corrections. Advanced imaging, such as 3D simulation, biochemical MRI, and MR arthrography with application of leg traction, has great potential to improve surgical decision-making. Further research is needed to assess the added clinical value of these techniques.
Keywords: MR arthrography; MRI; femoroacetabular impingement; imaging workup; radiography.
Figures

References
-
- Griffin DR, Dickenson EJ, O’Donnell J, et al. The Warwick agreement on femoroacetabular impingement syndrome (FAI syndrome): an international consensus statement. Br J Sports Med 2016; 50:1169–1176 - PubMed
-
- Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res 2003; 417:112–120 - PubMed
-
- Menge TJ, Briggs KK, Dornan GJ, McNamara SC, Philippon MJ. Survivorship and outcomes 10 years following hip arthroscopy for femoroacetabular impingement: labral debridement compared with labral repair. J Bone Joint Surg Am 2017; 99:997–1004 - PubMed
-
- Kaldau NC, Brorson S, Hölmich P, Lund B. Good midterm results of hip arthroscopy for femoroacetabular impingement. Dan Med J 2018; 65:A5483. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
