

Mammary Tumors Growing in the Absence of Growth Hormone Are More Sensitive to Doxorubicin Than Wild-Type Tumors
- PMID: 33475144
- PMCID: PMC7881836
- DOI: 10.1210/endocr/bqab013
Mammary Tumors Growing in the Absence of Growth Hormone Are More Sensitive to Doxorubicin Than Wild-Type Tumors
Abstract
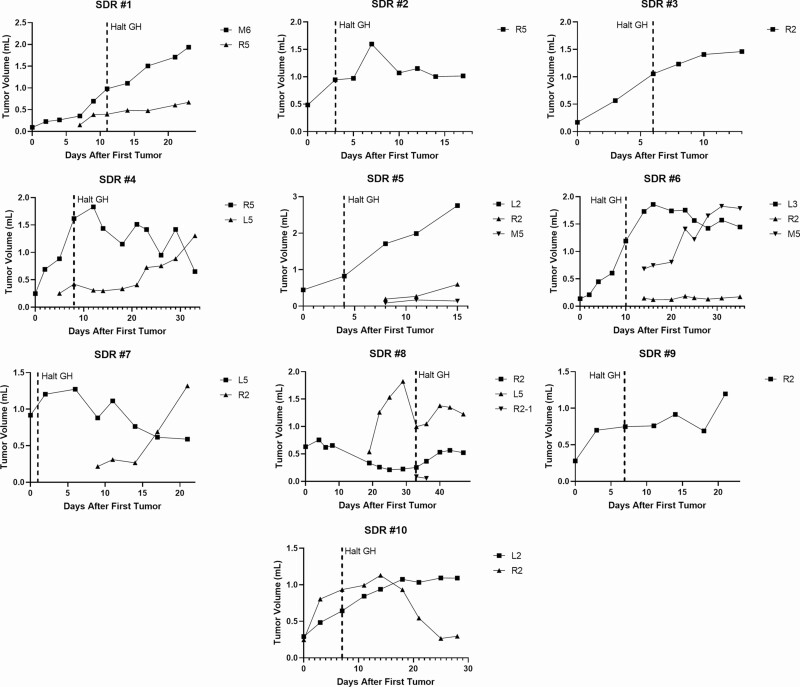
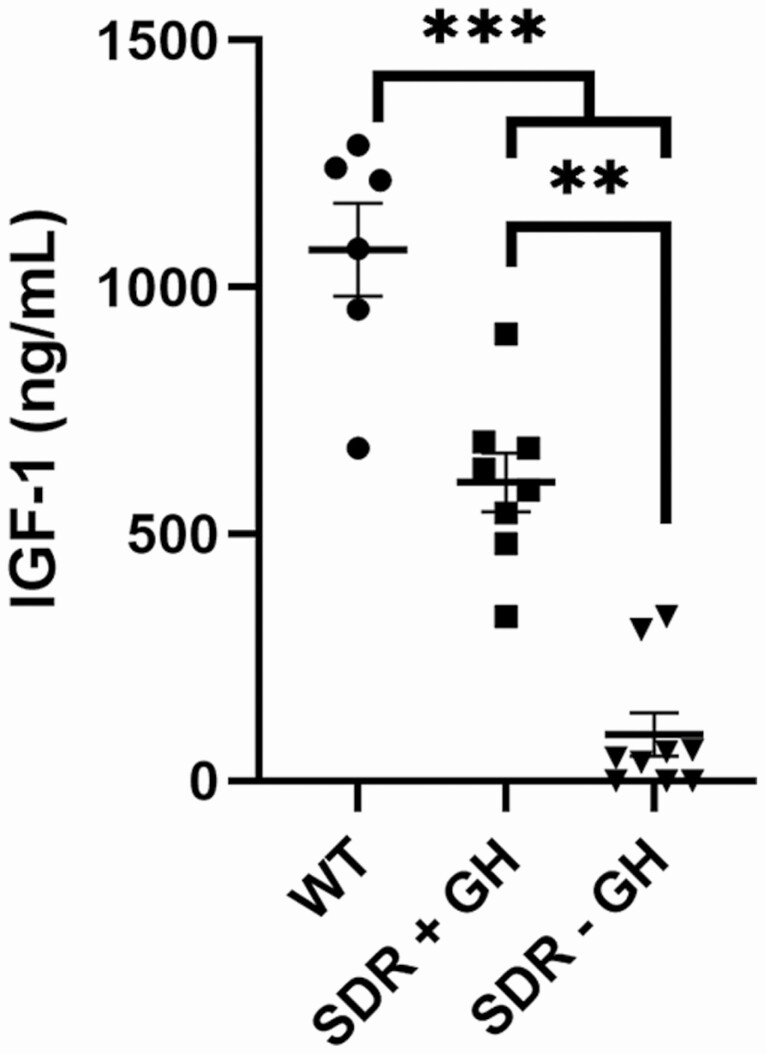
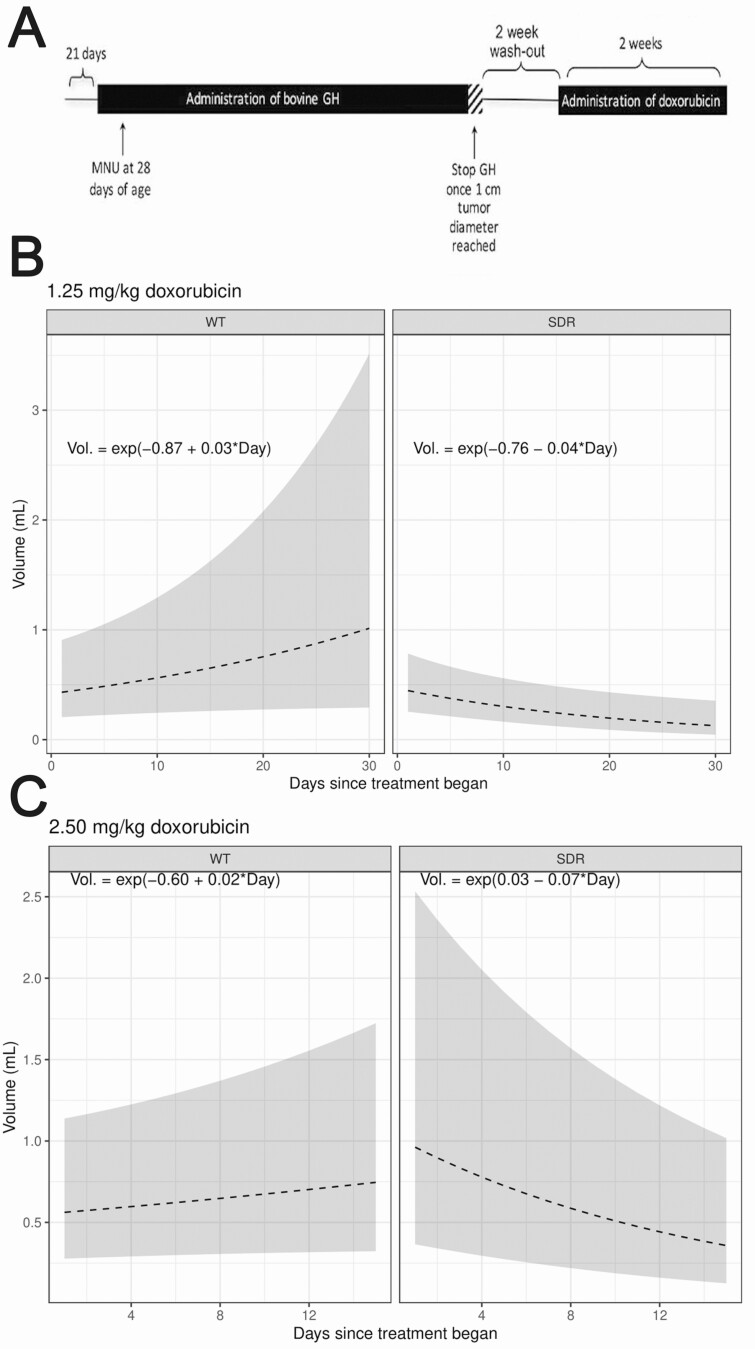
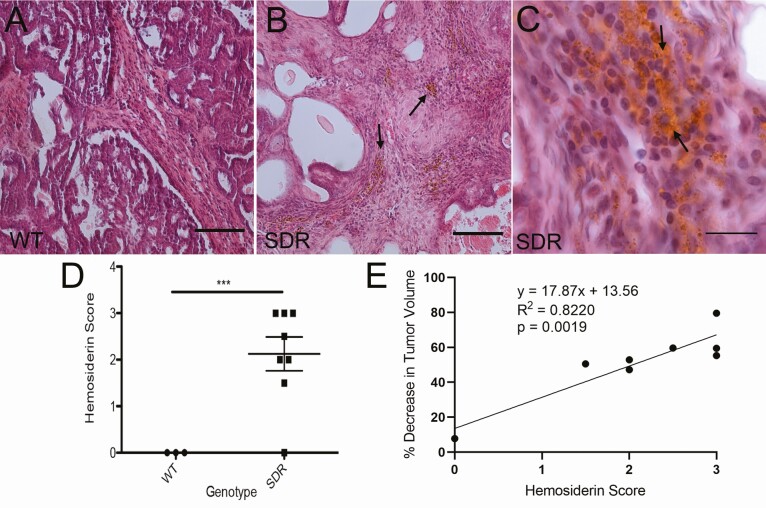
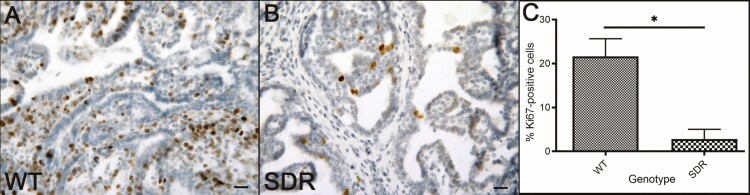
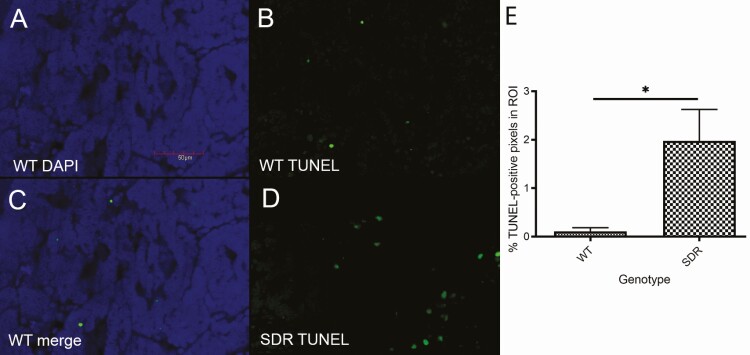
Previously, we reported that N-methyl-N-nitrosourea (MNU)-induced mammary tumors could be established in mutant spontaneous dwarf rats (SDRs), which lack endogenous growth hormone (GH) by supplementing with exogenous GH, and almost all such tumors regressed upon GH withdrawal. When the highly inbred SDR line was outcrossed to wild-type (WT) Sprague-Dawley rats, MNU-induced mammary tumors could still be established in resulting outbred SDRs by supplementing with exogenous GH. However, unlike tumors in inbred SDRs, 65% of mammary tumors established in outbred SDRs continued growth after GH withdrawal. We further tested whether these tumors were more sensitive to doxorubicin than their WT counterparts. To accomplish this, MNU-induced mammary tumors were established in WT rats and in SDRs supplemented with exogenous GH. Once mammary tumors reached 1 cm3 in size, exogenous GH was withdrawn from SDRs, and the subset that harbored tumors that continued or resumed growth in the absence of GH were selected for doxorubicin treatment. Doxorubicin was then administered in 6 injections over 2 weeks at 2.5 mg/kg or 1.25 mg/kg for both the WT and SDR groups. The SDR mammary tumors that had been growing in the absence of GH regressed at both doxorubicin doses while WT tumors continued to grow robustly. The regression of SDR mammary tumors treated with 1.25 mg/kg doxorubicin was accompanied by reduced proliferation and dramatically higher apoptosis relative to the WT mammary tumors treated with 1.25 mg/kg doxorubicin. These data suggest that downregulating GH signaling may decrease the doxorubicin dose necessary to effectively treat breast cancer.
Keywords: IGF-1; MNU; breast cancer; doxorubicin; growth hormone; mammary tumor.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Mammary tumorigenesis in growth hormone deficient spontaneous dwarf rats; effects of hormonal treatments.Breast Cancer Res Treat. 2004 Oct;87(3):277-90. doi: 10.1007/s10549-004-9504-2. Breast Cancer Res Treat. 2004. PMID: 15528971
-
The growth hormone-deficient Spontaneous Dwarf rat is resistant to chemically induced mammary carcinogenesis.Carcinogenesis. 2002 Jun;23(6):977-82. doi: 10.1093/carcin/23.6.977. Carcinogenesis. 2002. PMID: 12082019
-
Growth and characterization of N-methyl-N-nitrosourea-induced mammary tumors in intact and ovariectomized rats.Carcinogenesis. 2001 Dec;22(12):2039-47. doi: 10.1093/carcin/22.12.2039. Carcinogenesis. 2001. PMID: 11751437
-
Morphogenic and tumorigenic potentials of the mammary growth hormone/growth hormone receptor system.Mol Cell Endocrinol. 2002 Nov 29;197(1-2):153-65. doi: 10.1016/s0303-7207(02)00259-9. Mol Cell Endocrinol. 2002. PMID: 12431808 Review.
-
The contribution of growth hormone to mammary neoplasia.J Mammary Gland Biol Neoplasia. 2008 Mar;13(1):131-45. doi: 10.1007/s10911-008-9070-z. Epub 2008 Feb 7. J Mammary Gland Biol Neoplasia. 2008. PMID: 18253708 Free PMC article. Review.
Cited by
-
Mammary Tumor Growth and Proliferation Are Dependent on Growth Hormone in Female SV40 C3(1) T-Antigen Mice.Endocrinology. 2022 Dec 19;164(2):bqac174. doi: 10.1210/endocr/bqac174. Endocrinology. 2022. PMID: 36269749 Free PMC article.
-
Safety of growth hormone replacement in survivors of cancer and intracranial and pituitary tumours: a consensus statement.Eur J Endocrinol. 2022 Apr 21;186(6):P35-P52. doi: 10.1530/EJE-21-1186. Eur J Endocrinol. 2022. PMID: 35319491 Free PMC article. Review.
-
Growth Hormone Signaling in Bladder Cancer: Transcriptomic Profiling of Patient Samples and In Vitro Evidence of Therapy Resistance via ABC Transporters and EMT Activation.Int J Mol Sci. 2025 Jul 23;26(15):7113. doi: 10.3390/ijms26157113. Int J Mol Sci. 2025. PMID: 40806252 Free PMC article.
-
Covert actions of growth hormone: fibrosis, cardiovascular diseases and cancer.Nat Rev Endocrinol. 2022 Sep;18(9):558-573. doi: 10.1038/s41574-022-00702-6. Epub 2022 Jun 24. Nat Rev Endocrinol. 2022. PMID: 35750929 Free PMC article. Review.
-
Growth hormone receptor antagonism downregulates ATP-binding cassette transporters contributing to improved drug efficacy against melanoma and hepatocarcinoma in vivo.Front Oncol. 2022 Jul 5;12:936145. doi: 10.3389/fonc.2022.936145. eCollection 2022. Front Oncol. 2022. PMID: 35865483 Free PMC article.
References
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359-E386. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7-30. - PubMed
-
- Subramani R, Nandy SB, Pedroza DA, Lakshmanaswamy R. Role of growth hormone in breast cancer. Endocrinology. 2017;158(6):1543-1555. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
