

Long-term Safety and Efficacy of Etrasimod for Ulcerative Colitis: Results from the Open-label Extension of the OASIS Study
- PMID: 33475734
- PMCID: PMC8218705
- DOI: 10.1093/ecco-jcc/jjab016
Long-term Safety and Efficacy of Etrasimod for Ulcerative Colitis: Results from the Open-label Extension of the OASIS Study
Abstract
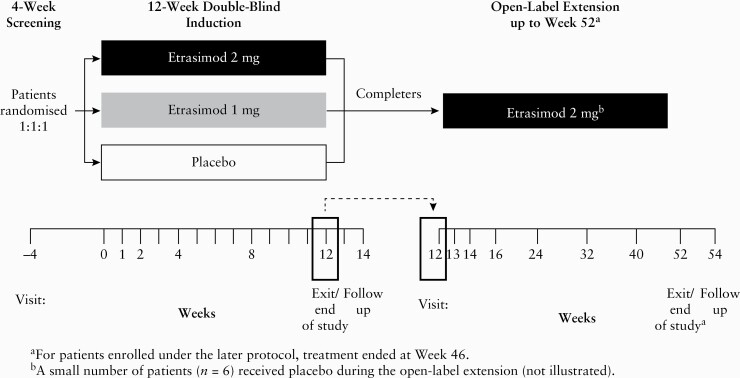
Background and aims: Etrasimod is an oral, selective, sphingosine 1-phosphate receptor modulator. In a phase 2, randomised, double-blind, placebo-controlled trial in adults with moderately-to-severely active ulcerative colitis [OASIS], etrasimod 2 mg provided significant benefit versus placebo and was generally well tolerated. This open-label extension [OLE] evaluated safety and efficacy of etrasimod for up to 52 weeks.
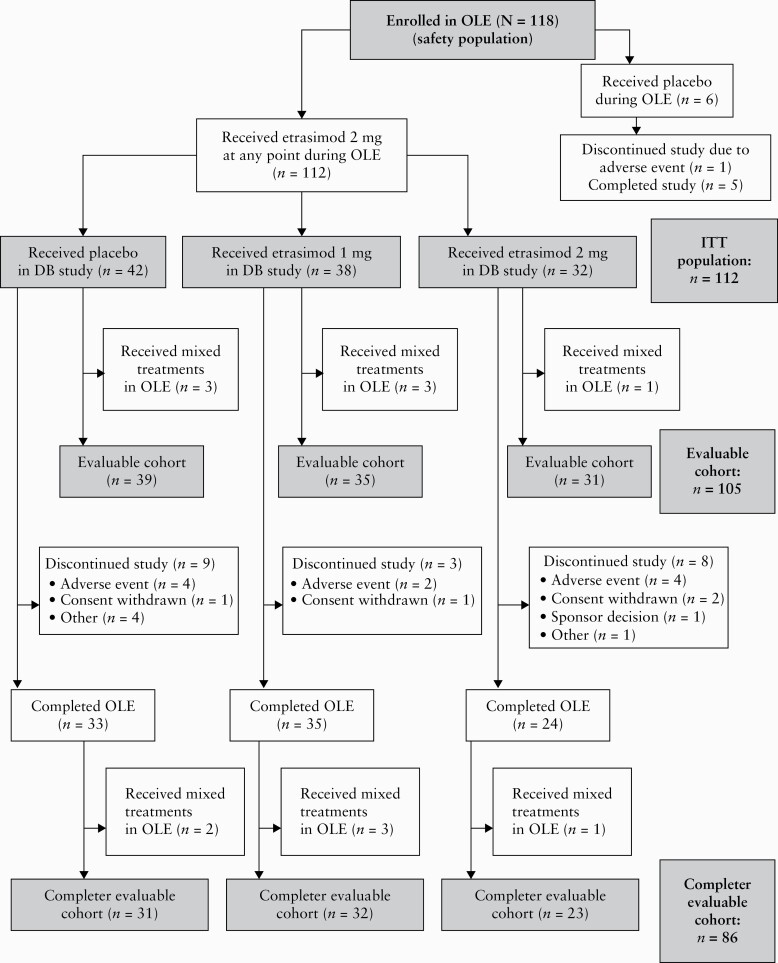
Methods: In OASIS, 156 patients received etrasimod 1 mg, etrasimod 2 mg, or placebo, once daily for 12 weeks. After completing OASIS, patients could enrol in the OLE and receive etrasimod 2 mg for an additional 34-40 weeks.
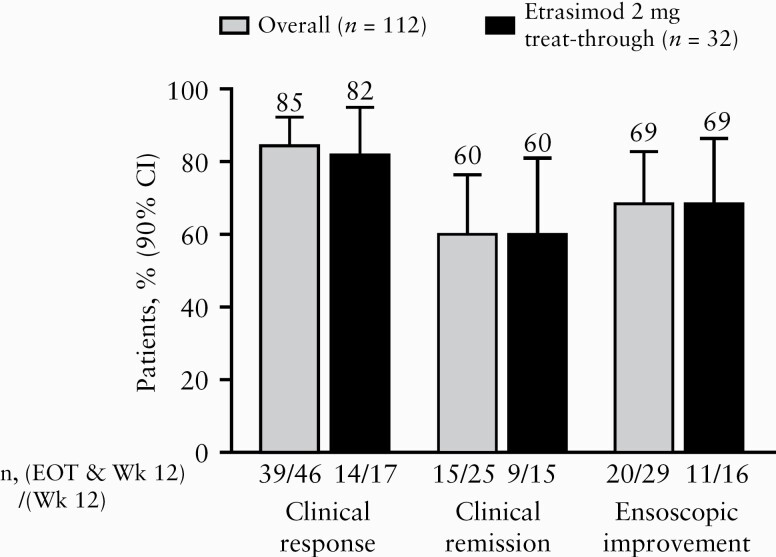
Results: In all, 118 patients enrolled in the OLE; 112 patients received etrasimod 2 mg at any point and were evaluated for safety and efficacy. A total of 92 [82%] patients who received etrasimod 2 mg in the OLE completed the study. Treatment-emergent adverse events occurred in 60% [67/112] of patients receiving etrasimod 2 mg at any time, most commonly worsening ulcerative colitis and anaemia; 94% of adverse events were mild/moderate. At end of treatment, 64% of patients met the criteria for clinical response, 33% for clinical remission, and 43% for endoscopic improvement. Week 12 clinical response, clinical remission, or endoscopic improvement was maintained to end of treatment in 85%, 60%, or 69% of patients, respectively. Steroid-free clinical remission occurred in 22% of overall patients.
Conclusions: In this long-term extension study, etrasimod 2 mg demonstrated a favourable safety profile. Most patients with clinical response, clinical remission, or endoscopic improvement at Week 12 maintained that status to end of treatment.
Keywords: Ulcerative colitis; etrasimod; long-term extension study.
© The Author(s) 2021. Published by Oxford University Press on behalf of European Crohn’s and Colitis Organisation.
Figures
References
-
- Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol 2019;114:384–413. - PubMed
-
- Harbord M, Eliakim R, Bettenworth D; European Crohn’s and Colitis Organisation . Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 2: current management. J Crohns Colitis 2017;11:769–84. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
