

Assessment of the Patient Protection and Affordable Care Act's Increase in Fees for Primary Care and Access to Care for Dual-Eligible Beneficiaries
- PMID: 33475756
- PMCID: PMC7821030
- DOI: 10.1001/jamanetworkopen.2020.33424
Assessment of the Patient Protection and Affordable Care Act's Increase in Fees for Primary Care and Access to Care for Dual-Eligible Beneficiaries
Abstract
Importance: The Patient Protection and Affordable Care Act (ACA) temporarily increased primary care practitioners' (PCP) Medicaid fees to that of Medicare for 2013 to 2014 (fee bump) to help accommodate potential increases in demand for care with ACA coverage expansion. This also increased fees for PCPs treating dual-eligible Medicare and Medicaid beneficiaries in many states and eliminated payment differentials for dual-eligible vs non-dual-eligible Medicare beneficiaries that could limit access to care.
Objective: To examine the association between the ACA fee bump and primary care visits for dual-eligible Medicare and Medicaid beneficiaries.
Design, setting, and participants: This cohort study used a difference-in-difference design and Medicare claims data from 2012 to 2016 to compare changes in visit rates for full-subsidy dual-eligible Medicare and Medicaid beneficiaries vs non-dual-eligible Medicare beneficiaries with low income whose fees did not change. Changes were examined overall and separately in states with temporary, extended, or minimal fee increases for dual-eligible vs non-dual-eligible beneficiaries in 2013 to 2014 (mandatory bump) and 2015 to 2016 (postbump or bump extension) vs 2012 (prebump). The study used linear regression models with beneficiary fixed effects, adjusting for time-changing area and beneficiary characteristics. Statistical analysis was performed from February 2018 to November 2019.
Exposure: ACA-mandated Medicaid fee bump.
Main outcomes and measures: Primary care visits per 100 beneficiaries overall and visits billed by physicians vs nurse practitioners and physician assistants.
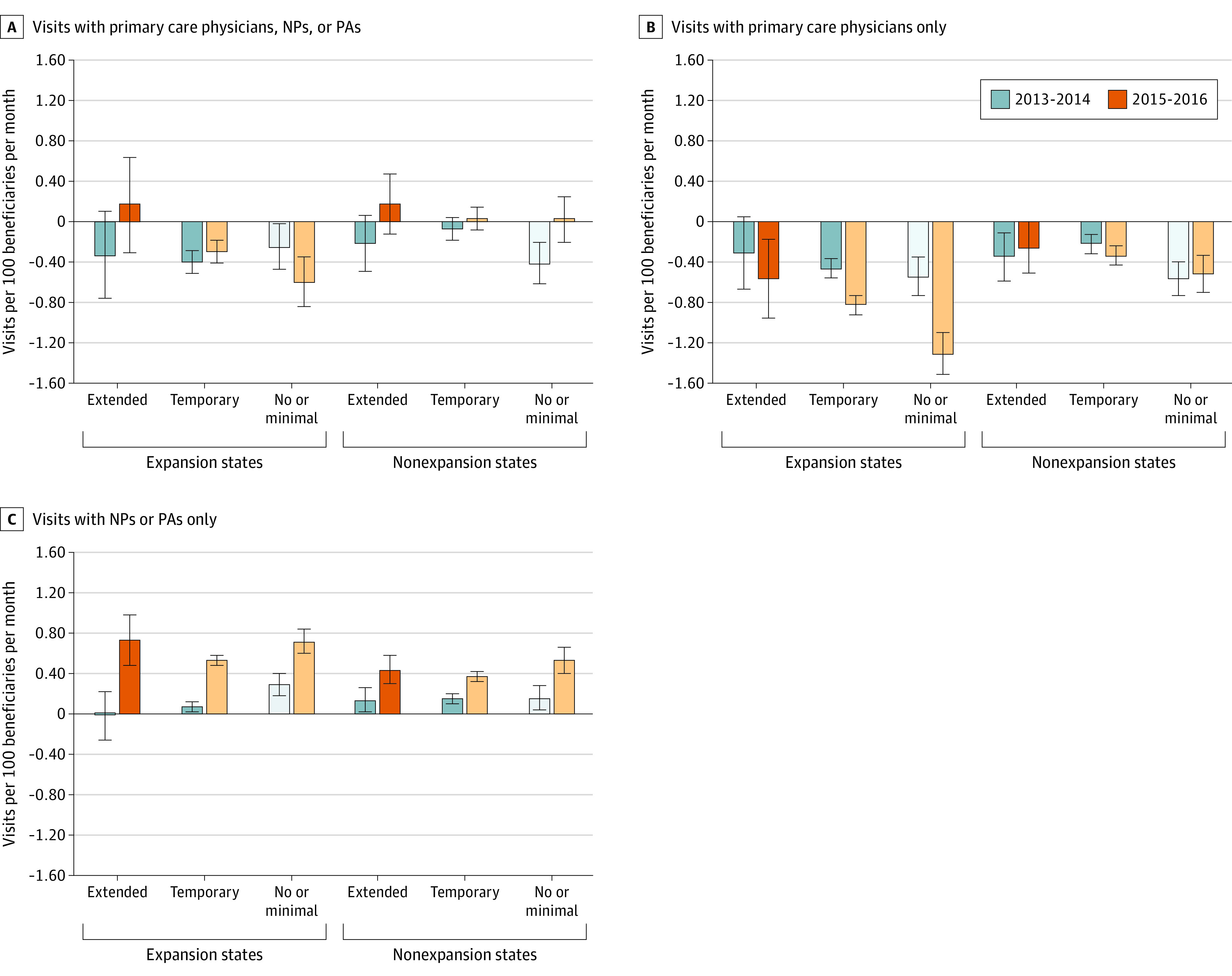
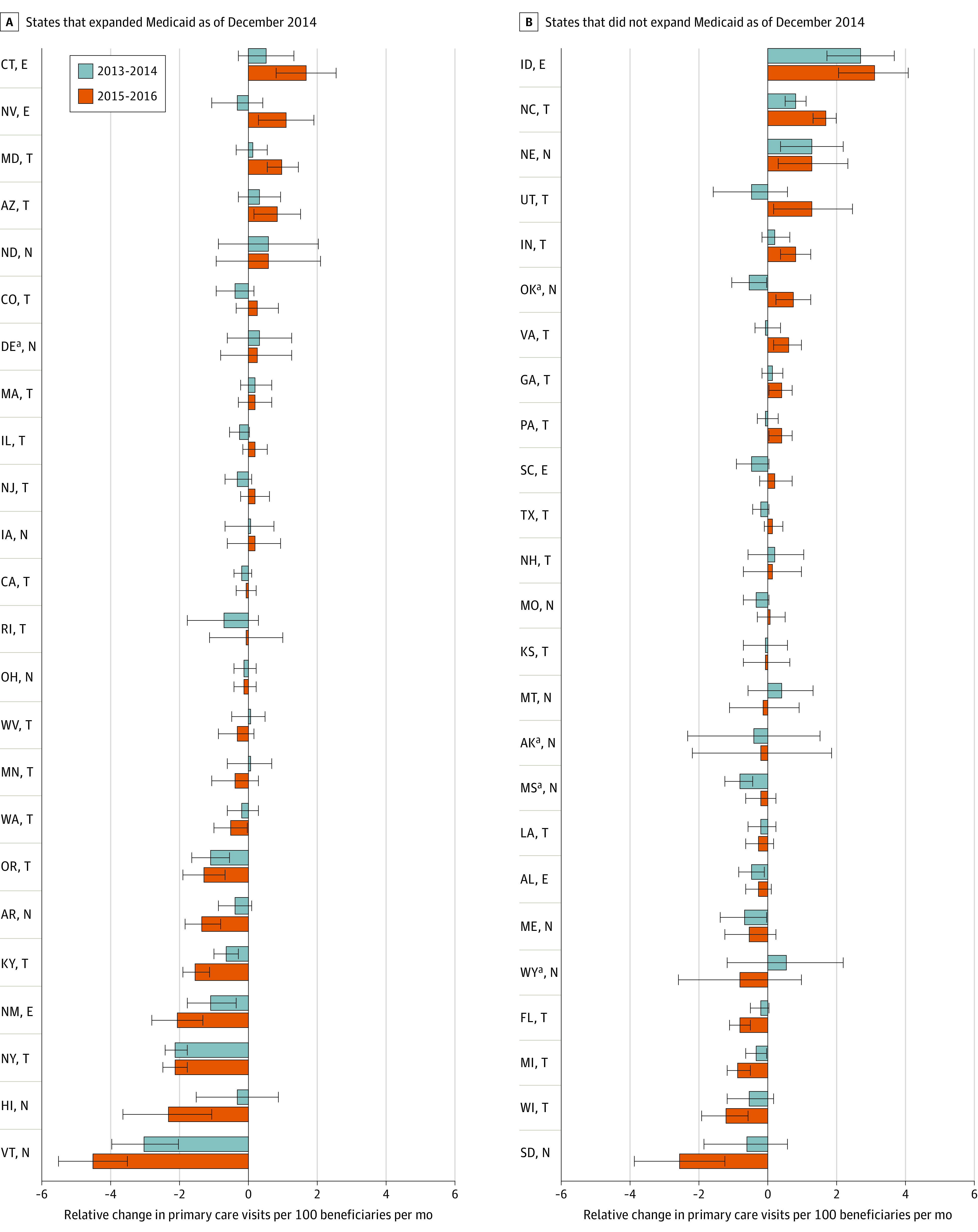
Results: The study included 3 052 044 dual-eligible and non-dual-eligible beneficiaries in 2012; 1 516 534 (49.7%) were aged 65 years or younger, 1 797 556 (58.9%) were women, and 1 754 626 (57.5%) had non-Hispanic White race/ethnicity. Overall primary care visit rates for dual-eligible beneficiaries were unchanged or decreased slightly relative to non-dual-eligible beneficiaries during the fee bump (2013-2014) and the postbump or bump extension period (2015-2016) vs baseline. Compared with non-dual-eligible beneficiaries, visit rates with primary care physicians declined more uniformly for dual-eligible beneficiaries across state groups and time periods (difference-in-difference: -0.37 [95% CI, -0.43 to -0.32] visits per 100 beneficiaries in 2013-2014 vs 2012; P < .001; and difference-in-difference: -0.62 [95% CI, -0.68 to -0.56] visits per 100 beneficiaries in 2015-2016 vs 2012; P < .001), whereas visits with nurse practitioners and physician assistants increased over time (difference-in-difference: 0.11 [95% CI, 0.08 to 0.14] visits per 100 beneficiaries in 2013-2014 vs 2012; P < .001; and difference-in-difference: 0.46 [95% CI, 0.43 to 0.50] visits per 100 beneficiaries in 2015-2016 vs 2012; P < .001). These changes, however, were not associated with the timing of the payment changes.
Conclusions and relevance: The ACA fee bump was not associated with increases in primary care visits for dual-eligible Medicare and Medicaid beneficiaries. Visits for dual-eligible beneficiaries with primary care physicians decreased after the ACA, a decrease that was partially offset by increases in visits with nonphysician clinicians.
Conflict of interest statement
Figures
Similar articles
-
Does Medicaid coverage of Medicare cost sharing affect physician care for dual-eligible Medicare beneficiaries?Health Serv Res. 2021 Jun;56(3):528-539. doi: 10.1111/1475-6773.13650. Epub 2021 Mar 28. Health Serv Res. 2021. PMID: 33778957 Free PMC article.
-
Payment Discrepancies and Access to Primary Care Physicians for Dual-eligible Medicare-Medicaid Beneficiaries.Med Care. 2021 Jun 1;59(6):487-494. doi: 10.1097/MLR.0000000000001525. Med Care. 2021. PMID: 33973937 Free PMC article.
-
No Association Found Between The Medicaid Primary Care Fee Bump And Physician-Reported Participation In Medicaid.Health Aff (Millwood). 2018 Jul;37(7):1092-1098. doi: 10.1377/hlthaff.2018.0078. Health Aff (Millwood). 2018. PMID: 29985691
-
The Impact of Changes in Medicaid Provider Fees on Provider Participation and Enrollees' Care: a Systematic Literature Review.J Gen Intern Med. 2019 Oct;34(10):2200-2209. doi: 10.1007/s11606-019-05160-x. Epub 2019 Aug 6. J Gen Intern Med. 2019. PMID: 31388912 Free PMC article.
-
Quality, Spending, Utilization, and Outcomes Among Dual-Eligible Medicare-Medicaid Beneficiaries in Integrated Care Programs: A Systematic Review.JAMA Health Forum. 2024 Jul 5;5(7):e242187. doi: 10.1001/jamahealthforum.2024.2187. JAMA Health Forum. 2024. PMID: 39028653 Free PMC article.
Cited by
-
Does Medicaid coverage of Medicare cost sharing affect physician care for dual-eligible Medicare beneficiaries?Health Serv Res. 2021 Jun;56(3):528-539. doi: 10.1111/1475-6773.13650. Epub 2021 Mar 28. Health Serv Res. 2021. PMID: 33778957 Free PMC article.
-
What Interventions Work to Reduce Cost Barriers to Primary Healthcare in High-Income Countries? A Systematic Review.Int J Environ Res Public Health. 2024 Aug 5;21(8):1029. doi: 10.3390/ijerph21081029. Int J Environ Res Public Health. 2024. PMID: 39200639 Free PMC article.
-
Food insecurity of people with disabilities who were Medicare beneficiaries during the COVID-19 pandemic.Disabil Health J. 2021 Oct;14(4):101166. doi: 10.1016/j.dhjo.2021.101166. Epub 2021 Jul 5. Disabil Health J. 2021. PMID: 34272190 Free PMC article.
-
The Impact of the Medicaid Reimbursement Bump on Influenza Vaccination Rates Among US Teens: Evidence from the National Immunization Survey-Teen 2011-2020.J Am Board Fam Med. 2024 Mar 11;37(1):137-146. doi: 10.3122/jabfm.2023.230170R2. J Am Board Fam Med. 2024. PMID: 38467428 Free PMC article.
References
-
- Congressional Budget Office Dual-eligible beneficiaries of Medicare and Medicaid: characteristics, health care spending, and evolving policies. Published June 2013. Accessed December 13, 2020. https://www.cbo.gov/sites/default/files/113th-congress-2013-2014/reports...
-
- Jiang HJ, Wier LM, Potter DEB, Burgess J Potentially preventable hospitalizations among Medicare-Medicaid dual eligibles, 2008: HCUP statistical brief #96. Agency for Healthcare Research and Quality Published September 2010. Accessed December 30, 2020. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb96.pdf - PubMed
-
- Burke G, Prindiville K Improving the Qualified Medicare Benefit Program for dual eligibles. National Senior Citizens Law Center. Published November 2011. Accessed December 13, 2020. https://www.thescanfoundation.org/sites/default/files/nsclc_issue_brief_...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
