

Emergence of SARS-CoV-2 B.1.1.7 Lineage - United States, December 29, 2020-January 12, 2021
- PMID: 33476315
- PMCID: PMC7821772
- DOI: 10.15585/mmwr.mm7003e2
Emergence of SARS-CoV-2 B.1.1.7 Lineage - United States, December 29, 2020-January 12, 2021
Abstract
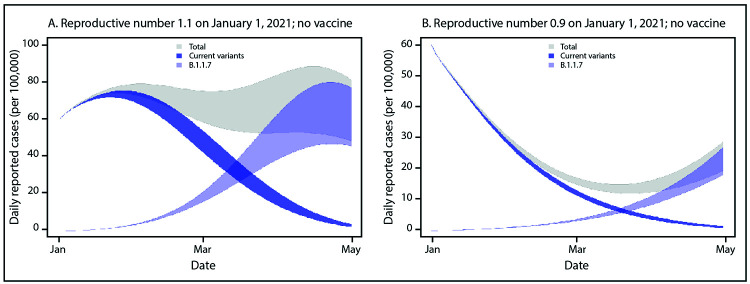
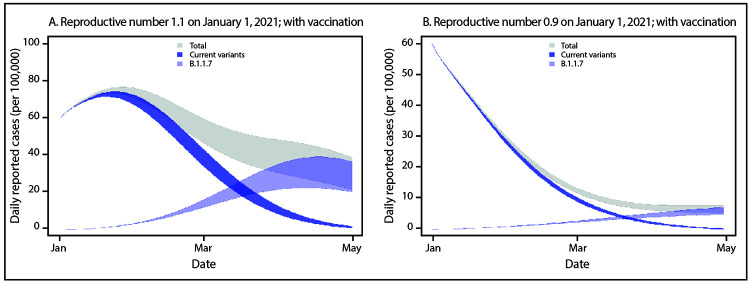
On December 14, 2020, the United Kingdom reported a SARS-CoV-2 variant of concern (VOC), lineage B.1.1.7, also referred to as VOC 202012/01 or 20I/501Y.V1.* The B.1.1.7 variant is estimated to have emerged in September 2020 and has quickly become the dominant circulating SARS-CoV-2 variant in England (1). B.1.1.7 has been detected in over 30 countries, including the United States. As of January 13, 2021, approximately 76 cases of B.1.1.7 have been detected in 12 U.S. states.† Multiple lines of evidence indicate that B.1.1.7 is more efficiently transmitted than are other SARS-CoV-2 variants (1-3). The modeled trajectory of this variant in the U.S. exhibits rapid growth in early 2021, becoming the predominant variant in March. Increased SARS-CoV-2 transmission might threaten strained health care resources, require extended and more rigorous implementation of public health strategies (4), and increase the percentage of population immunity required for pandemic control. Taking measures to reduce transmission now can lessen the potential impact of B.1.1.7 and allow critical time to increase vaccination coverage. Collectively, enhanced genomic surveillance combined with continued compliance with effective public health measures, including vaccination, physical distancing, use of masks, hand hygiene, and isolation and quarantine, will be essential to limiting the spread of SARS-CoV-2, the virus that causes coronavirus disease 2019 (COVID-19). Strategic testing of persons without symptoms but at higher risk of infection, such as those exposed to SARS-CoV-2 or who have frequent unavoidable contact with the public, provides another opportunity to limit ongoing spread.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
-
- Public Health England. Investigation of novel SARS-CoV-2 variant: variant of concern 202012/01, technical briefing 3. London, United Kingdom: Public Health England; 2020.. https://assets.publishing.service.gov.uk/government/uploads/system/uploa...
-
- Kemp SA, Harvey WT, Datir RP, et al. Recurrent emergence and transmission of a SARS-CoV-2 spike deletion ΔH69/V70. bioRxiv [Preprint posted online January 14, 2021]. https://www.biorxiv.org/content/10.1101/2020.12.14.422555v4 - DOI
-
- Volz E, Mishra S, Chand M, et al. Transmission of SARS-CoV-2 lineage B.1.1.7 in England: insights from linking epidemiological and genetic data. medRxiv [Preprint posted online January 4, 2021]. https://www.medrxiv.org/content/10.1101/2020.12.30.20249034v2 - DOI
-
- Honein MA, Christie A, Rose DA, et al. ; CDC COVID-19 Response Team. Summary of guidance for public health strategies to address high levels of community transmission of SARS-CoV-2 and related deaths, December 2020. MMWR Morb Mortal Wkly Rep 2020;69:1860–7. 10.15585/mmwr.mm6949e2 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
