

Associations of maternal dietary inflammatory potential and quality with offspring birth outcomes: An individual participant data pooled analysis of 7 European cohorts in the ALPHABET consortium
- PMID: 33476335
- PMCID: PMC7819611
- DOI: 10.1371/journal.pmed.1003491
Associations of maternal dietary inflammatory potential and quality with offspring birth outcomes: An individual participant data pooled analysis of 7 European cohorts in the ALPHABET consortium
Abstract
Background: Adverse birth outcomes are major causes of morbidity and mortality during childhood and associate with a higher risk of noncommunicable diseases in adult life. Maternal periconception and antenatal nutrition, mostly focusing on single nutrients or foods, has been shown to influence infant birth outcomes. However, evidence on whole diet that considers complex nutrient and food interaction is rare and conflicting. We aim to elucidate the influence of whole-diet maternal dietary inflammatory potential and quality during periconceptional and antenatal periods on birth outcomes.
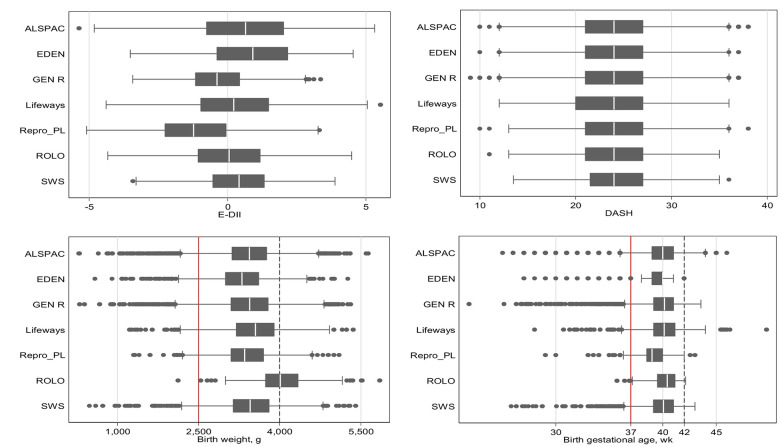
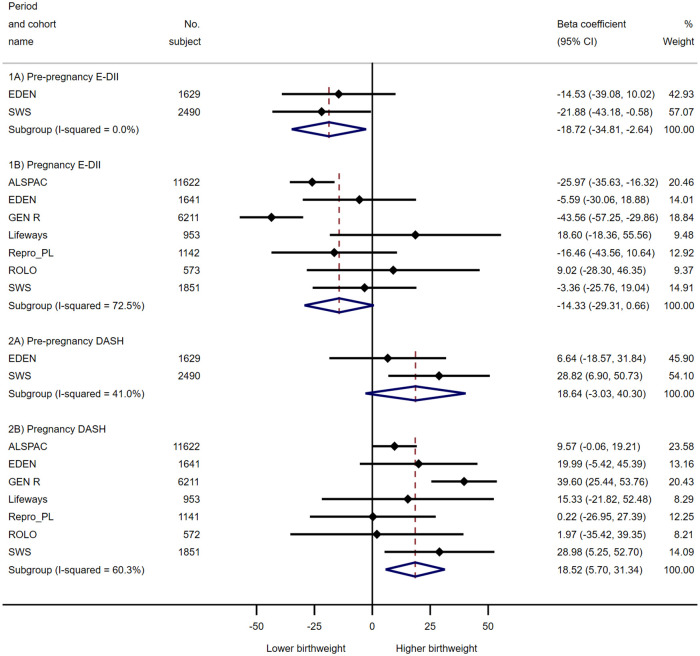
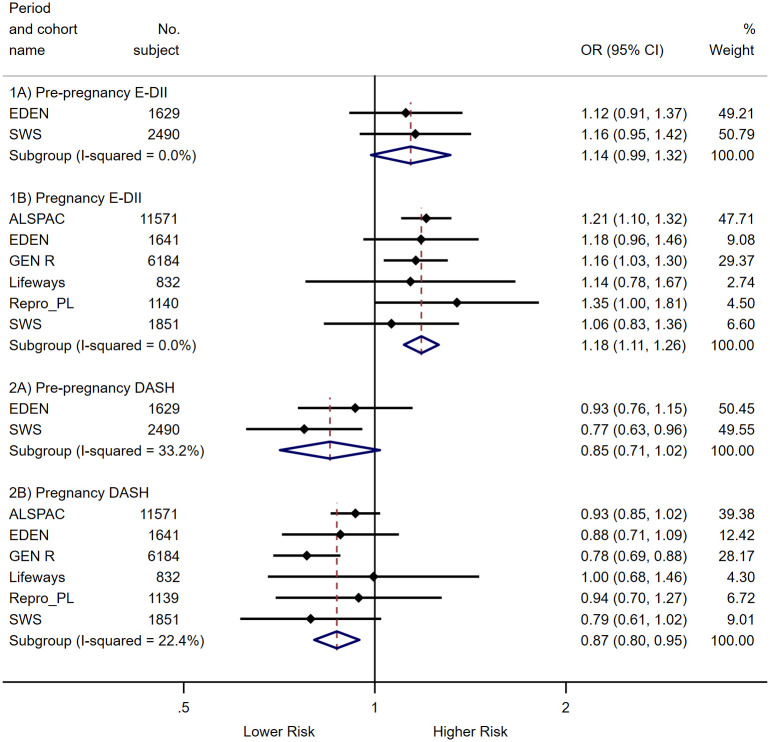
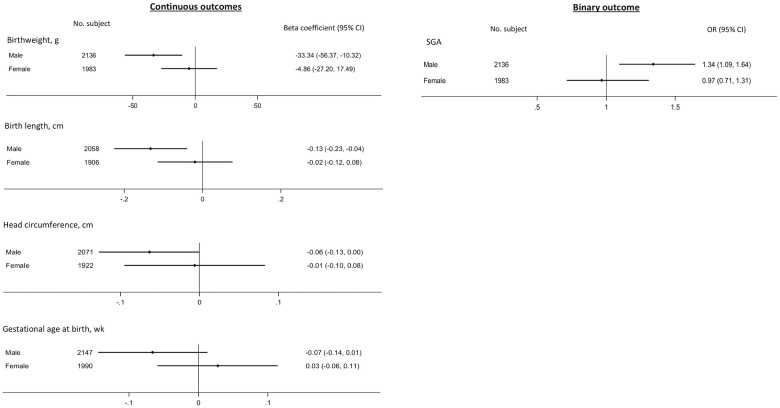
Methods and findings: We harmonized and pooled individual participant data (IPD) from up to 24,861 mother-child pairs in 7 European mother-offspring cohorts [cohort name, country (recruitment dates): ALSPAC, UK (1 April 1991 to 31 December 1992); EDEN, France (27 January 2003 to 6 March 2006); Generation R, the Netherlands (1 April 2002 to 31 January 2006); Lifeways, Ireland (2 October 2001 to 4 April 2003); REPRO_PL, Poland (18 September 2007 to 16 December 2011); ROLO, Ireland (1 January 2007 to 1 January 2011); SWS, United Kingdom (6 April 1998 to 17 December 2002)]. Maternal diets were assessed preconceptionally (n = 2 cohorts) and antenatally (n = 7 cohorts). Maternal dietary inflammatory potential and quality were ranked using the energy-adjusted Dietary Inflammatory Index (E-DII) and Dietary Approaches to Stop Hypertension (DASH) index, respectively. Primary outcomes were birth weight and gestational age at birth. Adverse birth outcomes, i.e., low birth weight (LBW), macrosomia, small-for-gestational-age (SGA), large-for-gestational-age (LGA), preterm and postterm births were defined according to standard clinical cutoffs. Associations of maternal E-DII and DASH scores with infant birth outcomes were assessed using cohort-specific multivariable regression analyses (adjusted for confounders including maternal education, ethnicity, prepregnancy body mass index (BMI), maternal height, parity, cigarettes smoking, and alcohol consumption), with subsequent random-effects meta-analyses. Overall, the study mothers had a mean ± SD age of 29.5 ± 4.9 y at delivery and a mean BMI of 23.3 ± 4.2 kg/m2. Higher pregnancy DASH score (higher dietary quality) was associated with higher birth weight [β(95% CI) = 18.5(5.7, 31.3) g per 1-SD higher DASH score; P value = 0.005] and head circumference [0.03(0.01, 0.06) cm; P value = 0.004], longer birth length [0.05(0.01, 0.10) cm; P value = 0.010], and lower risk of delivering LBW [odds ratio (OR) (95% CI) = 0.89(0.82, 0.95); P value = 0.001] and SGA [0.87(0.82, 0.94); P value < 0.001] infants. Higher maternal prepregnancy E-DII score (more pro-inflammatory diet) was associated with lower birth weight [β(95% CI) = -18.7(-34.8, -2.6) g per 1-SD higher E-DII score; P value = 0.023] and shorter birth length [-0.07(-0.14, -0.01) cm; P value = 0.031], whereas higher pregnancy E-DII score was associated with a shorter birth length [-0.06(-0.10, -0.01) cm; P value = 0.026] and higher risk of SGA [OR(95% CI) = 1.18(1.11, 1.26); P value < 0.001]. In male, but not female, infants higher maternal prepregnancy E-DII was associated with lower birth weight and head circumference, shorter birth length, and higher risk of SGA (P-for-sex-interaction = 0.029, 0.059, 0.104, and 0.075, respectively). No consistent associations were observed for maternal E-DII and DASH scores with gestational age, preterm and postterm birth, or macrosomia and LGA. Limitations of this study were that self-reported dietary data might have increased nondifferential measurement error and that causality cannot be claimed definitely with observational design.
Conclusions: In this cohort study, we observed that maternal diet that is of low quality and high inflammatory potential is associated with lower offspring birth size and higher risk of offspring being born SGA in this multicenter meta-analysis using harmonized IPD. Improving overall maternal dietary pattern based on predefined criteria may optimize fetal growth and avert substantial healthcare burden associated with adverse birth outcomes.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: JRH owns controlling interest in Connecting Health Innovations LLC (CHI), a company that has licensed the right to his invention of the dietary inflammatory index (DII) from the University of South Carolina in order to develop computer and smart phone applications for patient counselling and dietary intervention in clinical settings. NS is an employee of CHI. All other authors declare no support from any organisation for the submitted work other than those described above; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Galal M, Symonds I, Murray H, Petraglia F, Smith R. Postterm pregnancy. Facts, views Vis ObGyn. 2012;4: 175–87. Available http://www.ncbi.nlm.nih.gov/pubmed/24753906. - PMC - PubMed
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller A-B, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379: 2162–2172. Available: http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)60820-... 10.1016/S0140-6736(12)60820-4 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- MC_UP_A620_1015/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/2/MRC_/Medical Research Council/United Kingdom
- MC_U147585819/MRC_/Medical Research Council/United Kingdom
- MC_PC_21001/MRC_/Medical Research Council/United Kingdom
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- MC_PC_15018/MRC_/Medical Research Council/United Kingdom
- BB/P028179/1/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
- G0400491/MRC_/Medical Research Council/United Kingdom
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
- BB/P028187/1/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
- G9815508/MRC_/Medical Research Council/United Kingdom
- MC_U147585827/MRC_/Medical Research Council/United Kingdom
- MC_PC_21000/MRC_/Medical Research Council/United Kingdom
- 10/33/04/DH_/Department of Health/United Kingdom
- MC_UU_12011/1/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
