

Intermediate-dose anticoagulation, aspirin, and in-hospital mortality in COVID-19: A propensity score-matched analysis
- PMID: 33476420
- PMCID: PMC8013588
- DOI: 10.1002/ajh.26102
Intermediate-dose anticoagulation, aspirin, and in-hospital mortality in COVID-19: A propensity score-matched analysis
Abstract
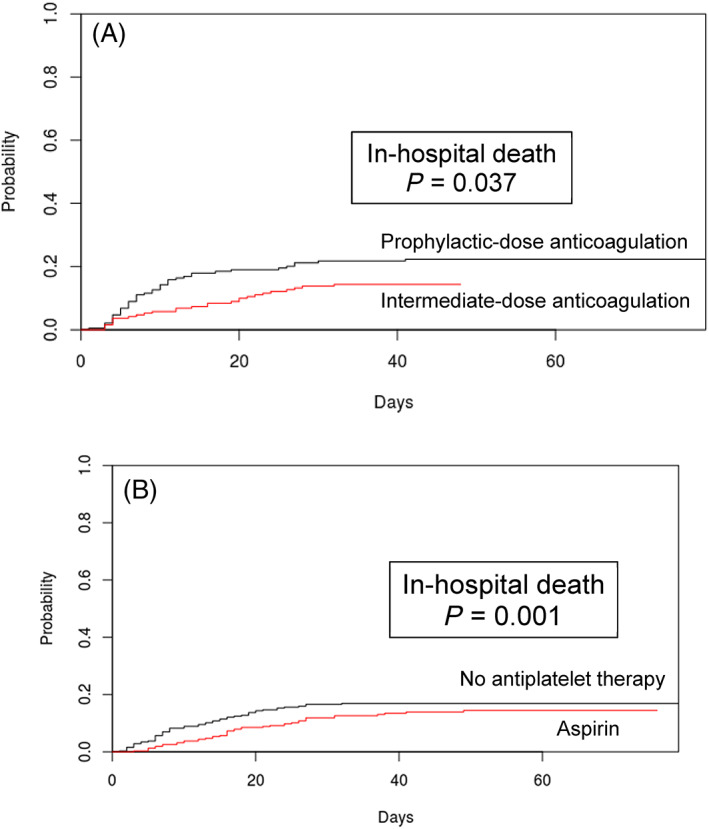
Thrombotic complications occur at high rates in hospitalized patients with COVID-19, yet the impact of intensive antithrombotic therapy on mortality is uncertain. We examined in-hospital mortality with intermediate- compared to prophylactic-dose anticoagulation, and separately with in-hospital aspirin compared to no antiplatelet therapy, in a large, retrospective study of 2785 hospitalized adult COVID-19 patients. In this analysis, we established two separate, nested cohorts of patients (a) who received intermediate- or prophylactic-dose anticoagulation ("anticoagulation cohort", N = 1624), or (b) who were not on home antiplatelet therapy and received either in-hospital aspirin or no antiplatelet therapy ("aspirin cohort", N = 1956). To minimize bias and adjust for confounding factors, we incorporated propensity score matching and multivariable regression utilizing various markers of illness severity and other patient-specific covariates, yielding treatment groups with well-balanced covariates in each cohort. The primary outcome was cumulative incidence of in-hospital death. Among propensity score-matched patients in the anticoagulation cohort (N = 382), in a multivariable regression model, intermediate- compared to prophylactic-dose anticoagulation was associated with a significantly lower cumulative incidence of in-hospital death (hazard ratio 0.518 [0.308-0.872]). Among propensity-score matched patients in the aspirin cohort (N = 638), in a multivariable regression model, in-hospital aspirin compared to no antiplatelet therapy was associated with a significantly lower cumulative incidence of in-hospital death (hazard ratio 0.522 [0.336-0.812]). In this propensity score-matched, observational study of COVID-19, intermediate-dose anticoagulation and aspirin were each associated with a lower cumulative incidence of in-hospital death.
© 2021 Wiley Periodicals LLC.
Conflict of interest statement
No conflict of interest exists for any author on this manuscript. This work was supported by a gift donation from Jack Levin and a separate anonymous donation to the Benign Hematology program at Yale, the DeLuca Foundation to fund hematology research at Yale, and the National Institutes of Health (grant HL142818 to H.J.C., and GM136651 and HL139116 to M.L.M.).
Figures
Update of
-
Intermediate-dose anticoagulation, aspirin, and in-hospital mortality in COVID-19: a propensity score-matched analysis.medRxiv [Preprint]. 2021 Jan 15:2021.01.12.21249577. doi: 10.1101/2021.01.12.21249577. medRxiv. 2021. Update in: Am J Hematol. 2021 Apr 1;96(4):471-479. doi: 10.1002/ajh.26102. PMID: 33469595 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical