

Timing and efficacy of mifepristone pretreatment for medical management of early pregnancy loss
- PMID: 33476659
- PMCID: PMC10302402
- DOI: 10.1016/j.contraception.2021.01.007
Timing and efficacy of mifepristone pretreatment for medical management of early pregnancy loss
Abstract
Objectives: To determine the time interval between mifepristone and misoprostol administration associated with the most efficacious early pregnancy loss (EPL) management.
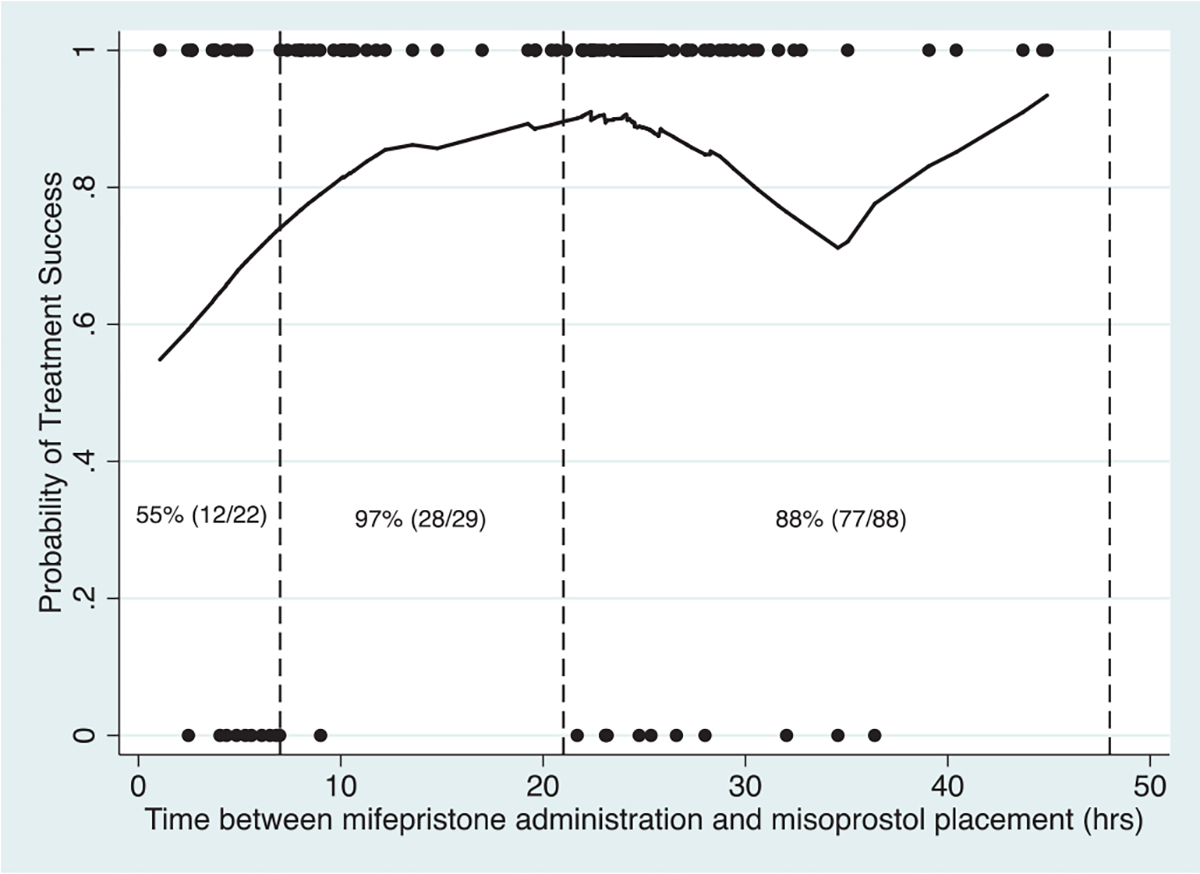
Study design: We performed a secondary analysis of a randomized trial. Participants with EPL were instructed to take 200 mg oral mifepristone followed by 800 mcg vaginal misoprostol 24 hours later. The primary outcome was gestational sac expulsion at the first follow-up visit (1-4 days after misoprostol use) after a single dose of misoprostol and no additional intervention within 30 days after treatment. Despite specification of drug timing, participants used the medication over a range of time. We graphed sliding average estimates of success and assessed the proportion of treatment successes over time to define timing interval cohorts for analysis. We used multivariable generalized linear regression to assess the association between time interval and success.
Results: Of 139 eligible participants, 70 (50.4%) self-administered misoprostol before 24 hours, and 69 (49.6%) at or after 24 hours. We defined the following time intervals: 0 to 6 hours (n = 22); 7 to 20 hours (n = 29); and 21 to 48 hours (n = 88). Success occurred in 96.6% of the 7- to 20-hour cohort compared to 54.6% and 87.5% of the cohorts self-administering misoprostol earlier or later, respectively. When adjusting for race, gestational age, diagnosis, bleeding at presentation, insurance status, and enrollment site, participants administering misoprostol between 0 and 6 hours (adjusted risk ratio 0.58, 95% CI 0.40-0.85) and 21 to 48 hours (adjusted risk ratio 0.91, 95% CI 0.72-0.99) had a lower risk of success when compared to participants administering 7 to 20 hours after mifepristone.
Conclusions: These data suggest that medical management of EPL has the highest likelihood of success when misoprostol is self-administered 7 to 20 hours after mifepristone.
Implications: These preliminary data suggest that patients have the highest likelihood of success when misoprostol is taken between 7 and 20 hours after mifepristone. In contrast with medical abortion, simultaneous medication administration may not be as effective as delayed. Future research is needed to confirm the optimal medication time interval.
Keywords: Early pregnancy loss; Medical management; Mifepristone; Miscarriage.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest: Dr Schreiber has received consulting fees from Danco laboratories. No other potential conflict of interest relevant to this article was reported.
Figures
References
-
- Ventura SJ, Curtin SC, Abma JC, Henshaw SK. Estimated pregnancy rates and rates of pregnancy outcomes for the United States, 1990–2008. Natl Vital Stat Rep 2012;60(7):1–21. - PubMed
-
- Prager S, Dalton V, Allen RH, American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins-Gynecology. ACOG Practice Bulletin No. 200: early pregnancy loss. Obstet Gynecol 2018;132(5):e197–207. - PubMed
-
- Gemzell-Danielsson K, Bygdeman M, Aronsson A. Studies on uterine contractility following mifepristone and various routes of misoprostol. Contraception 2006;74(1):31–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
