

Immunotherapy and Immunotherapy Combinations in Metastatic Castration-Resistant Prostate Cancer
- PMID: 33477569
- PMCID: PMC7831137
- DOI: 10.3390/cancers13020334
Immunotherapy and Immunotherapy Combinations in Metastatic Castration-Resistant Prostate Cancer
Abstract
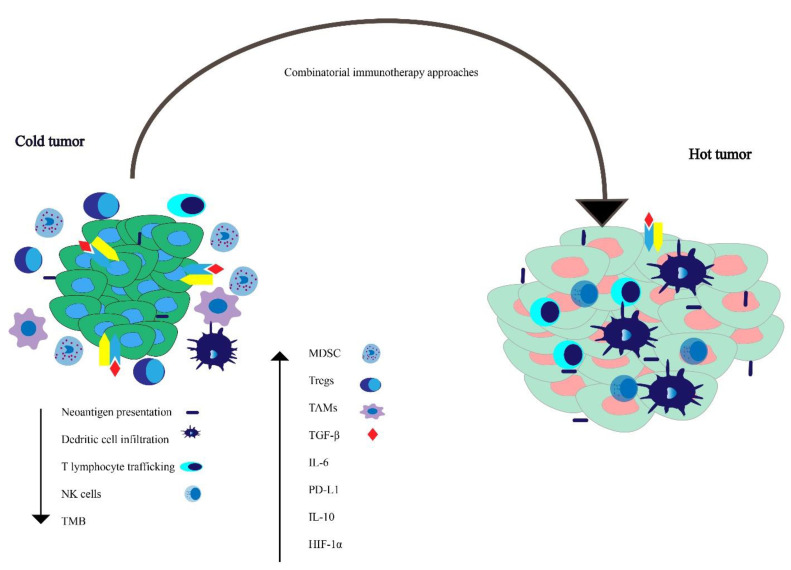
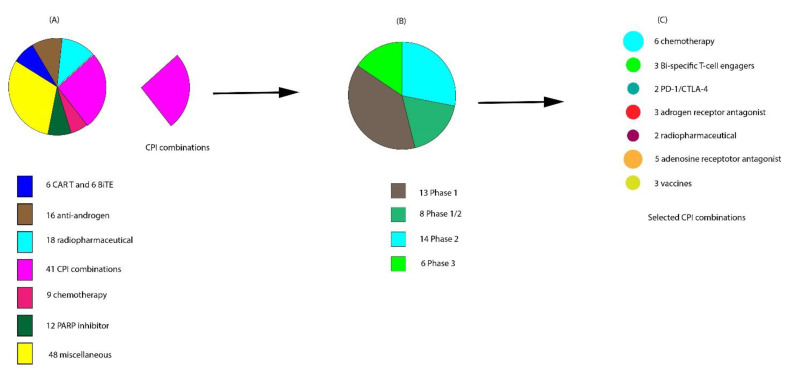
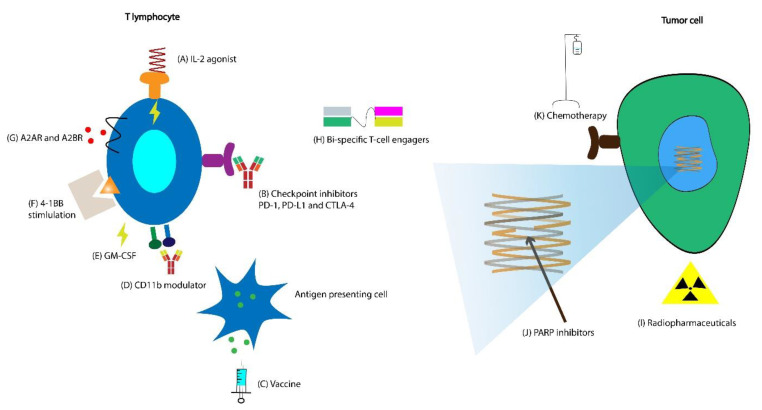
Although most prostate cancers are localized, and the majority are curable, recurrences occur in approximately 35% of men. Among patients with prostate-specific antigen (PSA) recurrence and PSA doubling time (PSADT) less than 15 months after radical prostatectomy, prostate cancer accounted for approximately 90% of the deaths by 15 years after recurrence. An immunosuppressive tumor microenvironment (TME) and impaired cellular immunity are likely largely responsible for the limited utility of checkpoint inhibitors (CPIs) in advanced prostate cancer compared with other tumor types. Thus, for immunologically "cold" malignancies such as prostate cancer, clinical trial development has pivoted towards novel approaches to enhance immune responses. Numerous clinical trials are currently evaluating combination immunomodulatory strategies incorporating vaccine-based therapies, checkpoint inhibitors, and chimeric antigen receptor (CAR) T cells. Other trials evaluate the efficacy and safety of these immunomodulatory agents' combinations with standard approaches such as androgen deprivation therapy (ADT), taxane-based chemotherapy, radiotherapy, and targeted therapies such as tyrosine kinase inhibitors (TKI) and poly ADP ribose polymerase (PARP) inhibitors. Here, we will review promising immunotherapies in development and ongoing trials for metastatic castration-resistant prostate cancer (mCRPC). These novel trials will build on past experiences and promise to usher a new era to treat patients with mCRPC.
Keywords: cancer vaccines; combination immunotherapy; immunotherapy; metastatic castrate-resistant prostate cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Howlader N.A., Krapcho M., Miller D., Brest A., Yu M., Ruhl J., Tatalovich Z., Mariotto A., Lewis D.R., Chen H.S., et al. 2018 Seer Data Submiss. National Cancer Institute; Bethesda, MD, USA: 2019. SEER Cancer Statistics Review, 1975–2016.
-
- Freedland S.J., Humphreys E.B., Mangold L.A., Eisenberger M., Dorey F.J., Walsh P.C., Partin A.W. Death in patients with recurrent prostate cancer after radical prostatectomy: Prostate-specific antigen doubling time subgroups and their associated contributions to all-cause mortality. J. Clin. Oncol. 2007;25:1765–1771. doi: 10.1200/JCO.2006.08.0572. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
