

Influence of Personality, Resilience and Life Conditions on Depression and Anxiety in 104 Patients Having Survived Acute Autoimmune Thrombotic Thrombocytopenic Purpura
- PMID: 33477992
- PMCID: PMC7835833
- DOI: 10.3390/jcm10020365
Influence of Personality, Resilience and Life Conditions on Depression and Anxiety in 104 Patients Having Survived Acute Autoimmune Thrombotic Thrombocytopenic Purpura
Abstract
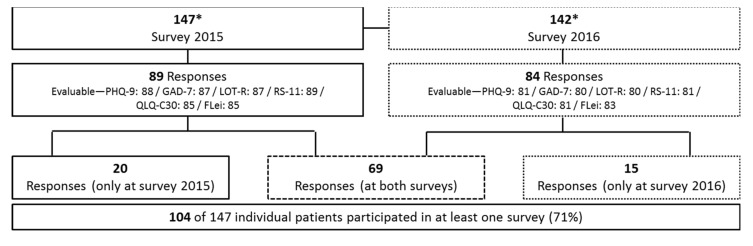
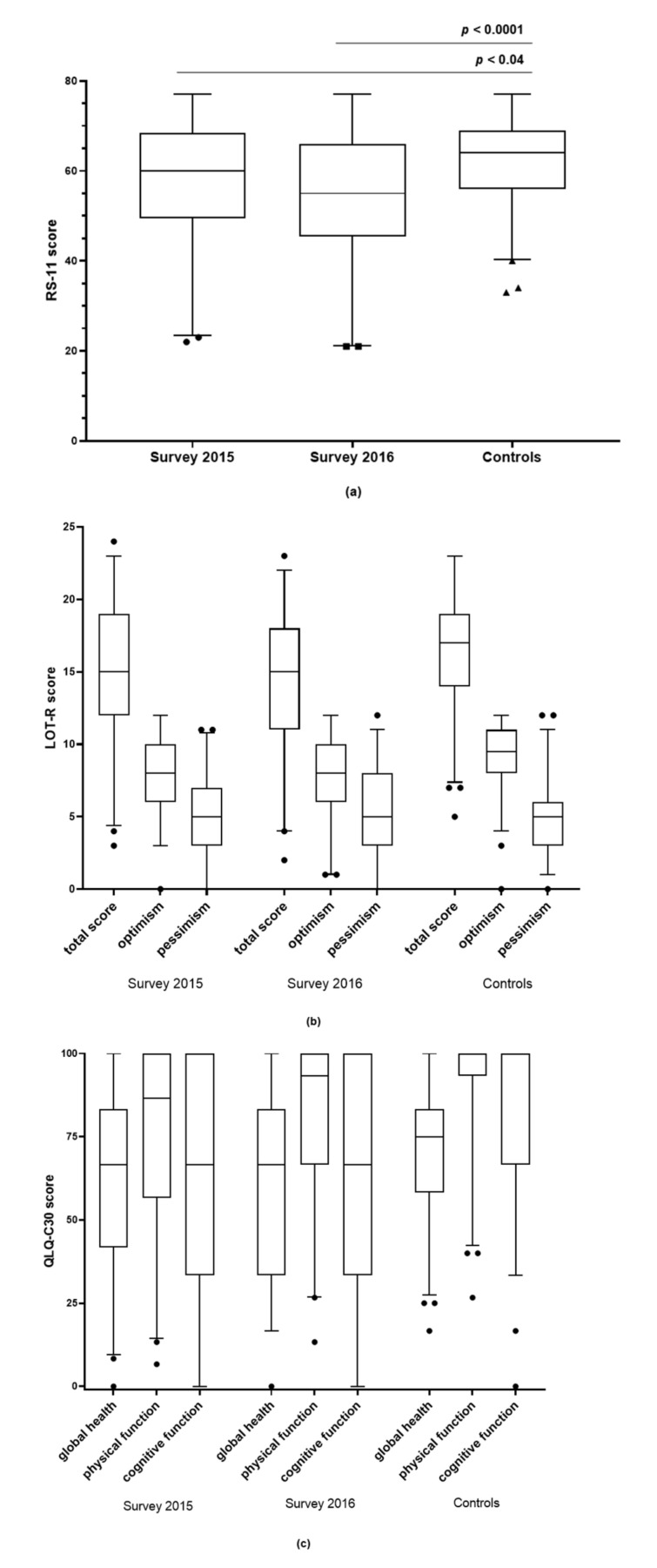
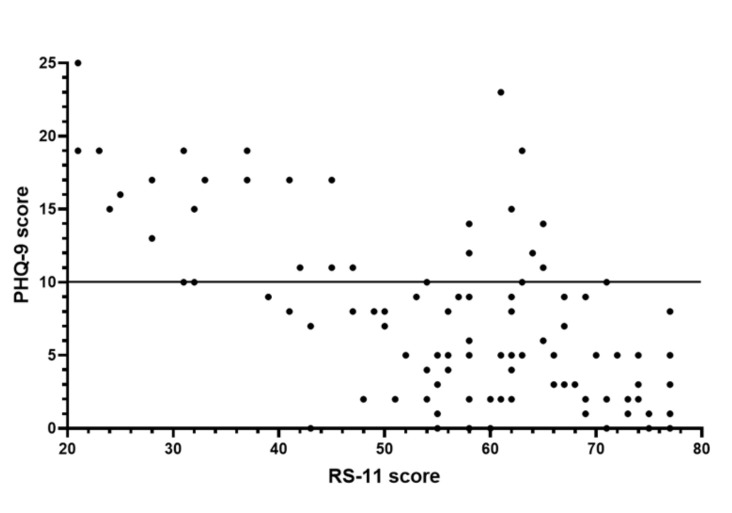
Autoimmune thrombotic thrombocytopenic purpura (iTTP) is a life-threatening, relapsing disease in which an acquired deficiency of the enzyme ADAMTS13 leads to generalised microvascular thrombosis. Survivors have a high prevalence of depression and impaired cognitive function. The aim of this study was to determine whether life circumstances and personality have an influence on the development and severity of depression and anxiety in iTTP patients and how they impact the quality of life. With validated questionnaires, we examined the prevalence of depression and anxiety symptoms in 104 iTTP patients, as well as parameters of subjective cognitive deficits, quality of life, attitude to life and resilience. iTTP patients had significantly more depressive symptoms (p < 0.001), a tendency to have anxiety disorders (p = 0.035) and a significantly worse cognitive performance (p = 0.008) compared to the controls. Sex, age, physical activity and partnership status had no significant influence on depression, whereas the number of comorbidities did. Lower scores of resilience, attitude to life and quality of life were reported by patients compared to controls. iTTP patients had a high prevalence of depression and anxiety, as well as a more negative attitude to life and low resilience. Resilience correlated negatively with the severity of the depression. Furthermore, quality of life and cognitive performance were significantly reduced.
Keywords: depression; quality of life; resilience; thrombotic thrombocytopenic purpura.
Conflict of interest statement
The authors state that they have no conflict of interest with this publication. Inge Scharrer is a member of the Data Safety Monitoring Board in the BAX 930 study (investigating recombi-nant ADAMTS13 infusion in hereditary TTP). Bernhard Lämmle is chairman of the Data Safety Monitoring Committee of the BAXALTA 281102 and the SHP655201 studies (now both run by TAKEDA), investigating recombinant ADAMTS13 in congenital and acquired TTP, respectively. He is on the Advisory Board of Sanofi for Caplacizumab, and received travel and accommodation support for participating at scientific meetings and/or lecture fees from Ablynx, Alexion, Siemens, Bayer, Roche, and Sanofi.
Figures

Similar articles
-
Long-term health-related quality of life and mental health in patients with immune thrombotic thrombocytopenic purpura.Ann Hematol. 2024 Jul;103(7):2523-2531. doi: 10.1007/s00277-024-05771-3. Epub 2024 Apr 27. Ann Hematol. 2024. PMID: 38671298 Free PMC article.
-
Survival after acute episodes of immune-mediated thrombotic thrombocytopenic purpura (iTTP) - cognitive functioning and health-related quality of life impact: a descriptive cross-sectional survey of adults living with iTTP in the United Kingdom.Hematology. 2021 Dec;26(1):465-472. doi: 10.1080/16078454.2021.1945236. Hematology. 2021. PMID: 34238132
-
Immune thrombotic thrombocytopenic purpura: Spotlight on long-term outcomes and survivorship.Front Med (Lausanne). 2023 Feb 28;10:1137019. doi: 10.3389/fmed.2023.1137019. eCollection 2023. Front Med (Lausanne). 2023. PMID: 36926315 Free PMC article. Review.
-
Multicenter Prospective Pilot Study Identifying Thrombomodulin as a Potential Biomarker for Neurocognitive Outcomes in Immune Thrombotic Thrombocytopenic Purpura.J Clin Med. 2025 Jan 22;14(3):694. doi: 10.3390/jcm14030694. J Clin Med. 2025. PMID: 39941363 Free PMC article.
-
Taking Empiricism out of Immune Thrombotic Thrombocytopenic Purpura: Current and Future Treatment Strategies.Transfus Med Rev. 2019 Oct;33(4):248-255. doi: 10.1016/j.tmrv.2019.06.005. Epub 2019 Aug 15. Transfus Med Rev. 2019. PMID: 31645275 Review.
Cited by
-
Special Issue: "The Latest Clinical Advances in Thrombocytopenia".J Clin Med. 2021 Aug 5;10(16):3463. doi: 10.3390/jcm10163463. J Clin Med. 2021. PMID: 34441759 Free PMC article.
-
TTP: From empiricism for an enigmatic disease to targeted molecular therapies.Br J Haematol. 2022 Apr;197(2):156-170. doi: 10.1111/bjh.18040. Epub 2022 Feb 10. Br J Haematol. 2022. PMID: 35146746 Free PMC article. Review.
-
Patient-Reported Outcome Measures in Patients with Thrombotic Thrombocytopenic Purpura: A Systematic Review of the Literature.J Clin Med. 2023 Aug 7;12(15):5155. doi: 10.3390/jcm12155155. J Clin Med. 2023. PMID: 37568558 Free PMC article. Review.
-
Integrating psychology services for patients with thrombotic thrombocytopenic purpura: A specialist centre experience.EJHaem. 2023 Jul 1;4(3):872-875. doi: 10.1002/jha2.726. eCollection 2023 Aug. EJHaem. 2023. PMID: 37601845 Free PMC article.
-
Long-term health-related quality of life and mental health in patients with immune thrombotic thrombocytopenic purpura.Ann Hematol. 2024 Jul;103(7):2523-2531. doi: 10.1007/s00277-024-05771-3. Epub 2024 Apr 27. Ann Hematol. 2024. PMID: 38671298 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
