

Adherence to prescription guidelines and achievement of treatment goals among persons with coronary heart disease in Tromsø 7
- PMID: 33478404
- PMCID: PMC7819182
- DOI: 10.1186/s12872-021-01866-1
Adherence to prescription guidelines and achievement of treatment goals among persons with coronary heart disease in Tromsø 7
Erratum in
-
Correction to: Adherence to prescription guidelines and achievement of treatment goals among persons with coronary heart disease in Tromsø 7.BMC Cardiovasc Disord. 2021 Aug 24;21(1):406. doi: 10.1186/s12872-021-02214-z. BMC Cardiovasc Disord. 2021. PMID: 34429065 Free PMC article. No abstract available.
Abstract
Background: Adherence to clinical practice guidelines for coronary heart disease (CHD) reduces morbidity, mortality and treatment costs. We aimed to describe and compare adherence to prescription guidelines for persons with CHD, and explore its association with treatment goal achievement.
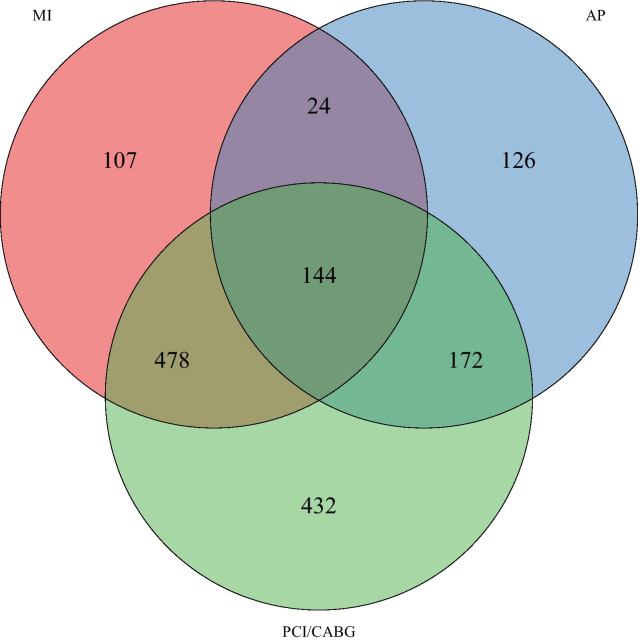
Method: We included all participants reporting myocardial infarction, angina, percutaneous coronary intervention and/or coronary artery bypass surgery in the seventh wave of the Tromsø Study (2015-2016, n = 1483). Medication use and treatment goal measures (blood pressure, low-density lipoprotein (LDL)-cholesterol and HbA1c) were compared to clinical practice guidelines on secondary CHD prevention. Propensity score matched logistic regression was used to assess the association between the use of antihypertensive drugs and achievement of treatment goal for blood pressure, and the use of lipid-lowering drugs (LLDs) and achievement of treatment goal for LDL-cholesterol.
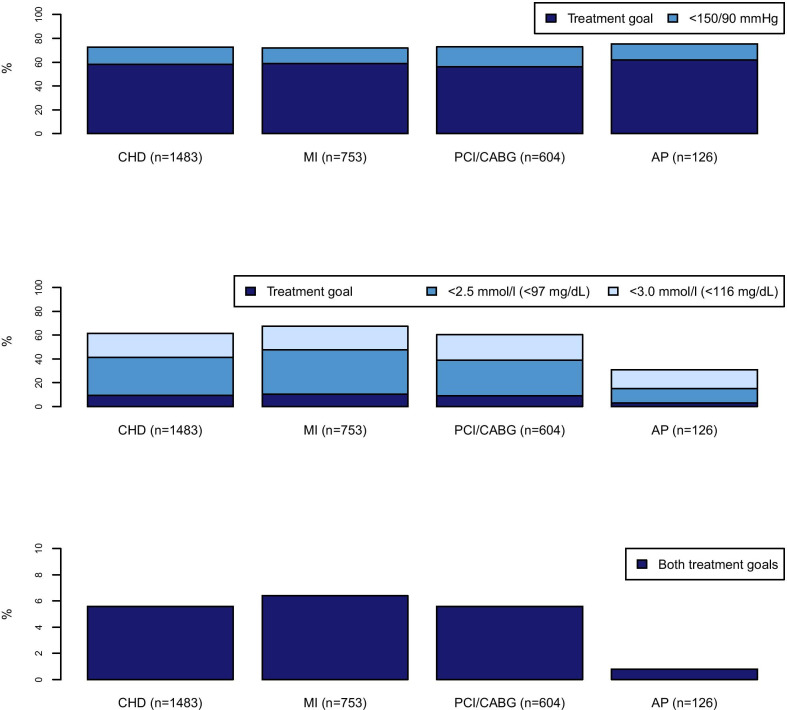
Results: The prevalence of pharmacological CHD treatment was 76% for LLDs, 72% for antihypertensive drugs and 66% for acetylsalicylic acid. The blood pressure goal (< 140/90 mmHg, < 140/80 mmHg if diabetic) was achieved by 58% and the LDL-cholesterol goal (< 1.8 mmol/l or < 70 mg/dL) by 9%. There was a strong association between using LLDs and achieving the treatment goal for LDL-cholesterol (OR 14.0, 95% CI 3.6-54.7), but not between using antihypertensive drugs and blood pressure goal achievement (OR 1.4, 95% CI 0.7-2.7).
Conclusion: Treatment goal achievement of LDL-cholesterol and blood pressure was low, despite the relatively high use of LLDs and antihypertensive drugs. Further research is needed to find the proper actions to increase achievement of the treatment goals.
Keywords: Antihypertensive agents; Blood pressure; Coronary heart disease; Lipid-lowering drugs; Low-density lipoprotein (LDL)-cholesterol; Prescription guidelines.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Naghavi MAA, Abbafati C, et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet (London, England) 2017;390(10100):1151–1210. doi: 10.1016/S0140-6736(17)32152-9. - DOI - PMC - PubMed
-
- Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet (London, England) 2004;364(9438):937–952. doi: 10.1016/S0140-6736(04)17018-9. - DOI - PubMed
-
- Mannsverk J, Wilsgaard T, Mathiesen EB, Lochen ML, Rasmussen K, Thelle DS, et al. Trends in modifiable risk factors are associated with declining incidence of hospitalized and nonhospitalized acute coronary heart disease in a population. Circulation. 2016;133(1):74–81. doi: 10.1161/CIRCULATIONAHA.115.016960. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
