

Factors associated with access and adherence to artemisinin-based combination therapy (ACT) for children under five: a secondary analysis of a national survey in Sierra Leone
- PMID: 33478507
- PMCID: PMC7817959
- DOI: 10.1186/s12936-021-03590-9
Factors associated with access and adherence to artemisinin-based combination therapy (ACT) for children under five: a secondary analysis of a national survey in Sierra Leone
Abstract
Background: Access and adherence to artemisinin-based combination therapy (ACT) are key challenges to effective malaria treatment. A secondary analysis of the Sierra Leone malaria Knowledge, Attitudes, and Practices (mKAP) survey was conducted to investigate access and adherence to ACT for the treatment of fever in children under-five.
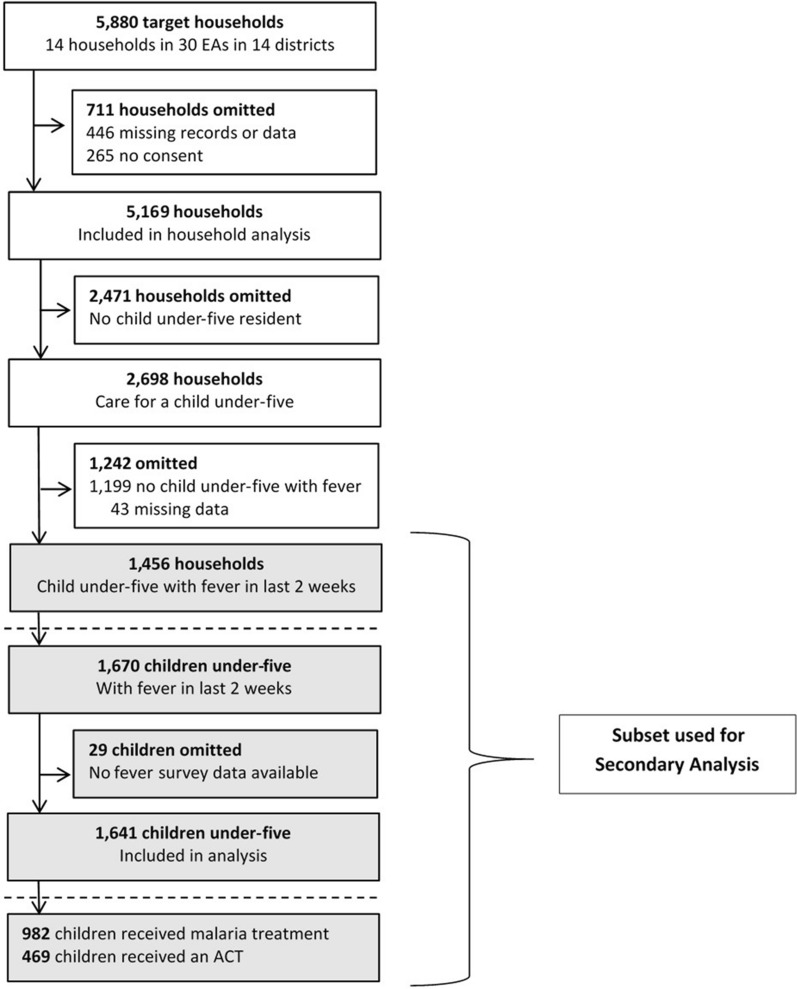
Methods: The mKAP was a nationally representative, two-stage cluster-sample survey, conducted in 2012. Thirty primary sampling units per district were randomly selected using probability proportionate to size, based on national census estimates; 14 households were subsequently randomly selected and enrolled per sampling unit. The analysis was restricted to children under-five with fever in the past two weeks. Factors associated with access and adherence were assessed using multivariate logistic regression.
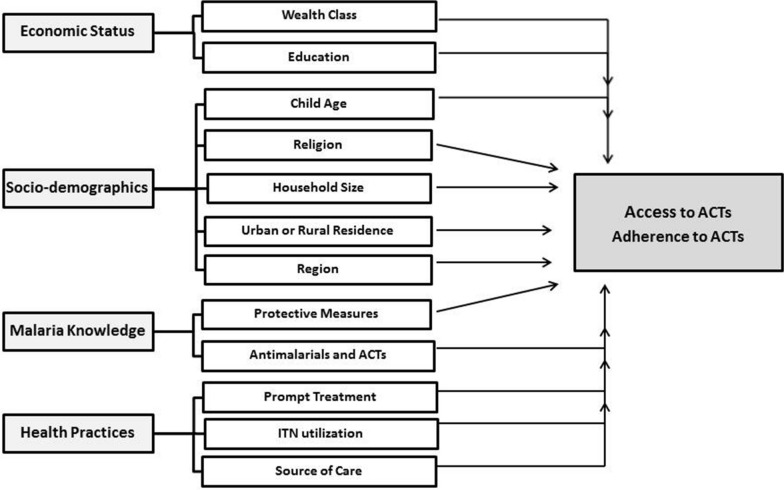
Results: Of 5169 enrolled households, 1456 reported at least one child under-five with fever in the past two weeks. Of the 1641 children from these households, 982 (59.8%) received any treatment for fever and were analysed for access to ACT; 469 (47.6%) received ACT and 466 were analysed for treatment adherence. Only 222 (47.4%) febrile children received ACT and completed 3-day treatment. In an adjusted analysis, factors associated with ACT access included knowledge of ACT (odds ratio [OR] 2.78, 95% CI 2.02-3.80; p < 0.001), knowledge of insecticide-treated nets (ITNs) (OR 1.84, 95% CI 1.29-2.63; p = 0.001), source of care (public health facility vs. other; OR 1.86, 95% CI 1.27-2.72, p = 0.001), geographic region (East vs. West; OR 2.30, 95% CI 1.20-4.44; p = 0.025), and age (24-59 vs. 0-23 months; OR 1.45, 95% CI 1.07-1.96; p = 0.016). The only factor associated with ACT adherence was time to treatment; children treated within 24 h were less likely to adhere (OR 0.55, 95% CI 0.34-0.89; p = 0.015).
Conclusions: In 2012, access and adherence to ACT remained low in Sierra Leone. Knowledge of ACT and ITNs, and seeking care in the public sector, were most strongly associated with ACT access. National surveys provide important information on anti-malarial access and could be expanded to measure treatment adherence.
Keywords: Access; Adherence; Antimalarial; Artemisinin-based combination therapy (ACT); Malaria; Prompt treatment; Sierra Leone; Treatment completion.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Caregivers' treatment-seeking behaviors and predictors of whether a child received an appropriate antimalarial treatment: a household survey in rural Uganda.BMC Infect Dis. 2016 Sep 6;16(1):478. doi: 10.1186/s12879-016-1815-5. BMC Infect Dis. 2016. PMID: 27600604 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Adherence to treatment with artemether-lumefantrine or amodiaquine-artesunate for uncomplicated malaria in children in Sierra Leone: a randomized trial.Malar J. 2018 Jun 4;17(1):222. doi: 10.1186/s12936-018-2370-x. Malar J. 2018. PMID: 29866192 Free PMC article. Clinical Trial.
-
Patterns and predictors of malaria care-seeking, diagnostic testing, and artemisinin-based combination therapy for children under five with fever in Northern Nigeria: a cross-sectional study.Malar J. 2014 Nov 21;13:447. doi: 10.1186/1475-2875-13-447. Malar J. 2014. PMID: 25413231 Free PMC article.
-
Paediatric formulations of artemisinin-based combination therapies for treating uncomplicated malaria in children.Cochrane Database Syst Rev. 2020 Dec 8;12(12):CD009568. doi: 10.1002/14651858.CD009568.pub2. Cochrane Database Syst Rev. 2020. PMID: 33289099 Free PMC article.
Cited by
-
Risk factors of malaria transmission in mining workers in Muara Enim, South Sumatra, Indonesia.Sci Rep. 2023 Sep 7;13(1):14755. doi: 10.1038/s41598-023-40418-9. Sci Rep. 2023. PMID: 37679466 Free PMC article.
-
Starting at the community: Treatment-seeking pathways of children with suspected severe malaria in Uganda.PLOS Glob Public Health. 2023 Jul 5;3(7):e0001949. doi: 10.1371/journal.pgph.0001949. eCollection 2023. PLOS Glob Public Health. 2023. PMID: 37405978 Free PMC article.
-
Comprehensive genomic study of Plasmodium falciparum in Sierra leone: genetic variation and resistance patterns.BMC Genomics. 2025 Jul 1;26(1):584. doi: 10.1186/s12864-025-11771-y. BMC Genomics. 2025. PMID: 40597624 Free PMC article.
-
Understanding Malaria Treatment Adherence in Rwanda: Implications for Artemisinin Resistance.medRxiv [Preprint]. 2025 Jul 23:2025.07.22.25331991. doi: 10.1101/2025.07.22.25331991. medRxiv. 2025. PMID: 40778167 Free PMC article. Preprint.
-
Evaluating recurrent episodes of malaria incidence in Timika, Indonesia, through a Markovian multiple-state model.Infect Dis Model. 2022 Jun 6;7(3):261-276. doi: 10.1016/j.idm.2022.05.008. eCollection 2022 Sep. Infect Dis Model. 2022. PMID: 35754556 Free PMC article.
References
-
- WHO . World malaria report 2017. Geneva: World Health Organization; 2017.
-
- WHO . World malaria report 2018. Geneva: World Health Organization; 2018.
-
- WHO . World malaria report 2019. Geneva: World Health Organization; 2019.
-
- WHO . Guidelines for the treatment of malaria. Third. Geneva: World Health Organization; 2015. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
