

The coArtHA trial-identifying the most effective treatment strategies to control arterial hypertension in sub-Saharan Africa: study protocol for a randomized controlled trial
- PMID: 33478567
- PMCID: PMC7818218
- DOI: 10.1186/s13063-021-05023-z
The coArtHA trial-identifying the most effective treatment strategies to control arterial hypertension in sub-Saharan Africa: study protocol for a randomized controlled trial
Abstract
Background: Arterial hypertension is the most prevalent risk factor for cardiovascular disease in sub-Saharan Africa. Only a few and mostly small randomized trials have studied antihypertensive treatments in people of African descent living in sub-Saharan Africa.
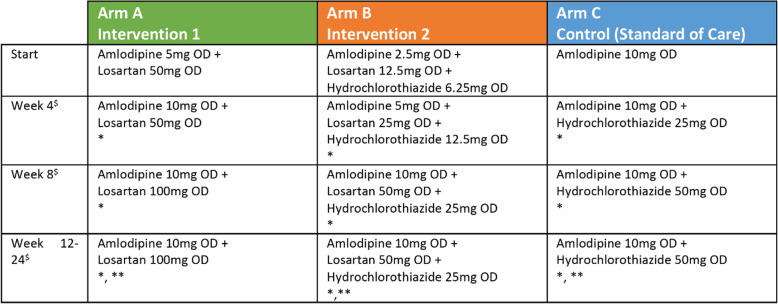
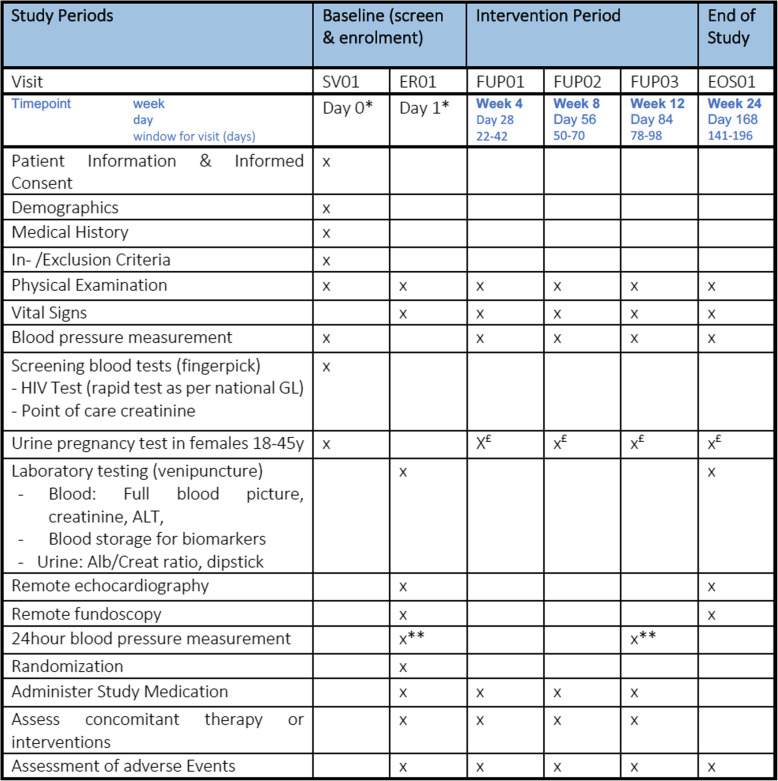
Methods: In this open-label, three-arm, parallel randomized controlled trial conducted at two rural hospitals in Lesotho and Tanzania, we compare the efficacy and cost-effectiveness of three antihypertensive treatment strategies among participants aged ≥ 18 years. The study includes patients with untreated uncomplicated arterial hypertension diagnosed by a standardized office blood pressure ≥ 140/90 mmHg. The trial encompasses a superiority comparison between a triple low-dose antihypertensive drug combination versus the current standard of care (monotherapy followed by dual treatment), as well as a non-inferiority comparison for a dual drug combination versus standard of care with optional dose titration after 4 and 8 weeks for participants not reaching the target blood pressure. The sample size is 1268 participants with parallel allocation and a randomization ratio of 2:1:2 for the dual, triple and control arms, respectively. The primary endpoint is the proportion of participants reaching a target blood pressure at 12 weeks of ≤ 130/80 mmHg and ≤ 140/90 mmHg among those aged < 65 years and ≥ 65 years, respectively. Clinical manifestations of end-organ damage and cost-effectiveness at 6 months are secondary endpoints.
Discussion: This trial will help to identify the most effective and cost-effective treatment strategies for uncomplicated arterial hypertension among people of African descent living in rural sub-Saharan Africa and inform future clinical guidelines on antihypertensive management in the region.
Trial registration: Clinicaltrials.gov NCT04129840 . Registered on 17 October 2019 ( https://www.clinicaltrials.gov/ ).
Keywords: Antihypertensive therapy; Arterial hypertension; Blood pressure; Dual therapy; HIV; Randomized controlled trial; Sub-Saharan Africa; Tanzania and Lesotho; Triple therapy.
Conflict of interest statement
All authors declare that they have no competing interests.
Figures
References
-
- Mokdad AH, Forouzanfar MH, Daoud F, Mokdad AA, El Bcheraoui C, Moradi-Lakeh M, et al. Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2016;387:2383–2401. doi: 10.1016/S0140-6736(16)00648-6. - DOI - PubMed
-
- WHO | Raised blood pressure. WHO n.d. https://www.who.int/gho/ncd/risk_factors/blood_pressure_prevalence_text/en/. (Accessed 26 Mar 2020).
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
