

Pathological Evidence for SARS-CoV-2 as a Cause of Myocarditis: JACC Review Topic of the Week
- PMID: 33478655
- PMCID: PMC7816957
- DOI: 10.1016/j.jacc.2020.11.031
Pathological Evidence for SARS-CoV-2 as a Cause of Myocarditis: JACC Review Topic of the Week
Abstract
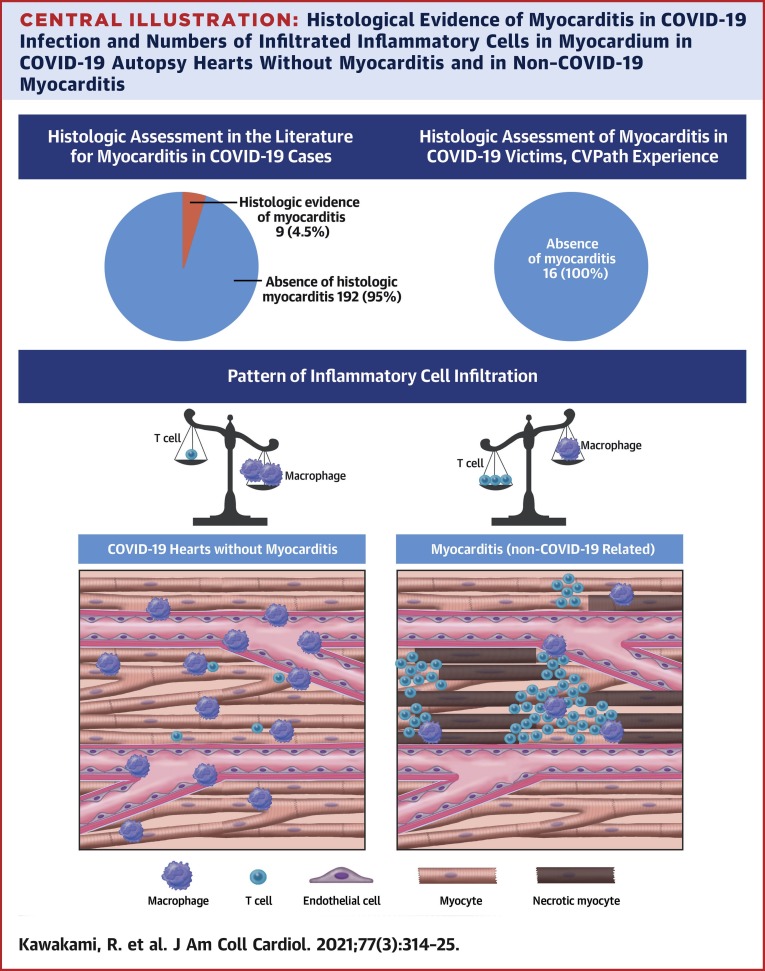
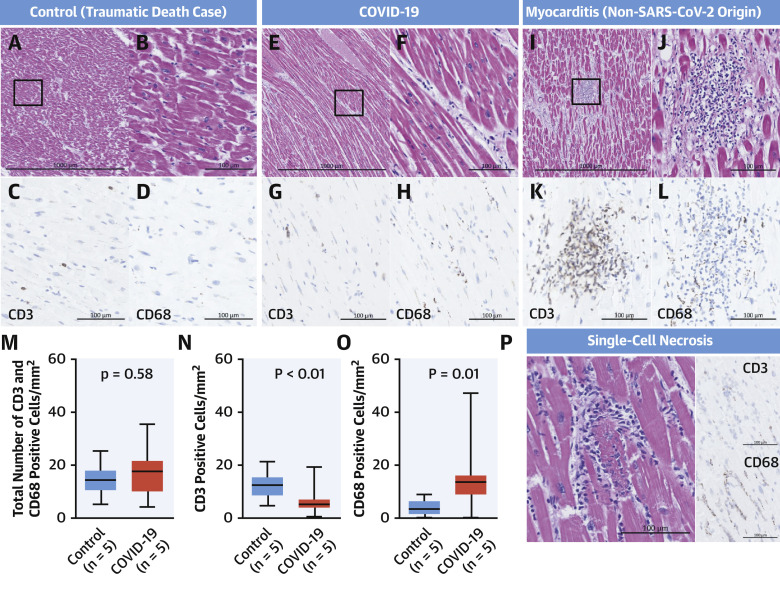
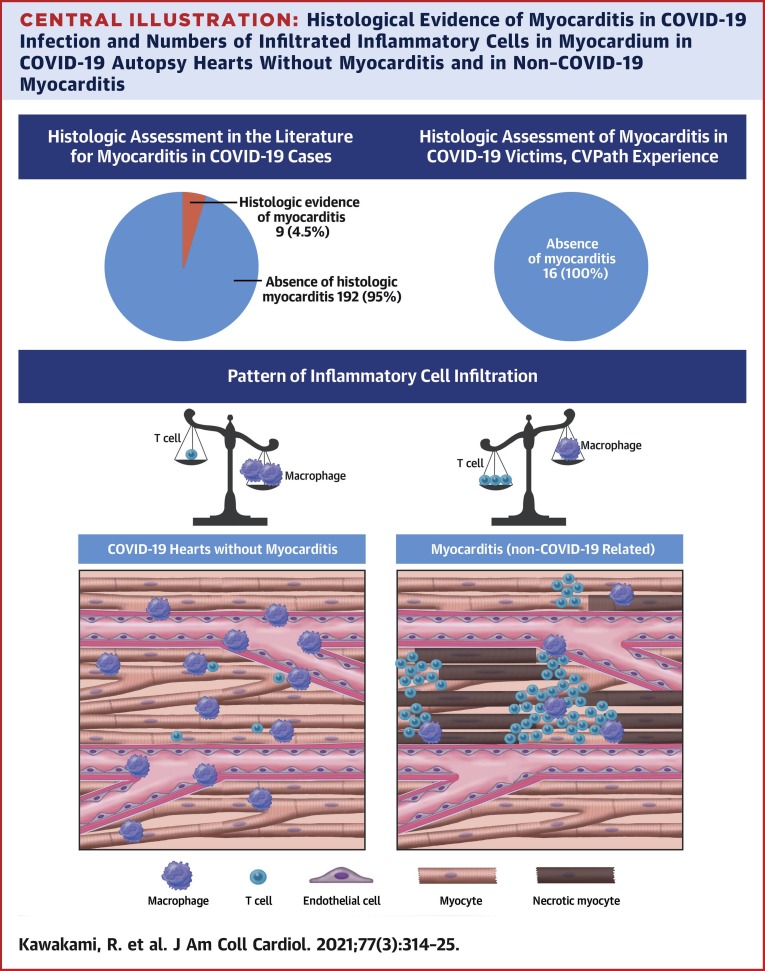
To investigate whether severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2)-induced myocarditis constitutes an important mechanism of cardiac injury, a review was conducted of the published data and the authors' experience was added from autopsy examination of 16 patients dying of SARS-CoV-2 infection. Myocarditis is an uncommon pathologic diagnosis occurring in 4.5% of highly selected cases undergoing autopsy or endomyocardial biopsy. Although polymerase chain reaction-detectable virus could be found in the lungs of most coronavirus disease-2019 (COVID-19)-infected subjects in our own autopsy registry, in only 2 cases was the virus detected in the heart. It should be appreciated that myocardial inflammation alone by macrophages and T cells can be seen in noninfectious deaths and COVID-19 cases, but the extent of each is different, and in neither case do such findings represent clinically relevant myocarditis. Given its extremely low frequency and unclear therapeutic implications, the authors do not advocate use of endomyocardial biopsy to diagnose myocarditis in the setting of COVID-19.
Keywords: COVID-19; SARS-CoV-2; cardiovascular disease; heart.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author Disclosures This study was supported by the CVPath Institute, a 501(c)(3) foundation. CVPath Institute has received institutional research support from R01 HL141425 Leducq Foundation Grant, 480 Biomedical, 4C Medical, 4Tech, Abbott, Accumedical, Amgen, Biosensors, Boston Scientific, Cardiac Implants, Celonova, Claret Medical, Concept Medical, Cook, CSI, DuNing, Inc, Edwards LifeSciences, Emboline, Endotronix, Envision Scientific, Lutonix/Bard, Gateway, Lifetech, Limflo, MedAlliance, Medtronic, Mercator, Merill, Microport Medical, Microvention, Mitralign, MitrAssist, NAMSA, Nanova, Neovasc, NIPRO, Novogate, Occulotech, OrbusNeich Medical, Phenox, Profusa, Protembis, Qool, Recor, Senseonics, Shockwave, Sinomed, Spectranetics, Surmodics, Symic, Vesper, W.L. Gore, and Xeltis. Dr. Cornelissen has received research grants from University Hospital RWTH Aachen. Dr. Guagliumi has received institutional research grants from Abbott Vascular, Boston Scientific, and Infraredx; and has served as a consultant for Abbott Vascular and Boston Scientific. Dr. Virmani has received honoraria from Abbott Vascular, Biosensors, Boston Scientific, Celonova, Cook Medical, Cordis, CSI, Lutonix Bard, Medtronic, OrbusNeich Medical, CeloNova, SINO Medical Technology, Recor Medical, Terumo Corporation, W. L. Gore, and Spectranetics; and has served as a consultant for Abbott Vascular, Boston Scientific, Celonova, Cook Medical, Cordis, CSI, Edwards Lifesciences, Lutonix Bard, Medtronic, OrbusNeich Medical, ReCore, Sinomedical Technology, Spectranetics, Surmodics, Terumo Corporation, W. L. Gore, and Xeltis. Dr. Finn has received honoraria from Abbott Vascular, Biosensors, Boston Scientific, Celonova, Cook Medical, CSI, Lutonix Bard, Sinomed, and Terumo Corporation; and has served as a consultant to Amgen, Abbott Vascular, Boston Scientific, Celonova, Cook Medical, Lutonix Bard, and Sinomed. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
