

Quantified health and cost effects of faster endovascular treatment for large vessel ischemic stroke patients in the Netherlands
- PMID: 33479037
- PMCID: PMC8606465
- DOI: 10.1136/neurintsurg-2020-017017
Quantified health and cost effects of faster endovascular treatment for large vessel ischemic stroke patients in the Netherlands
Abstract
Background: The effectiveness of endovascular treatment (EVT) for large vessel occlusion (LVO) stroke severely depends on time to treatment. However, it remains unclear what the value of faster treatment is in the years after index stroke. The aim of this study was to quantify the value of faster EVT in terms of health and healthcare costs for the Dutch LVO stroke population.
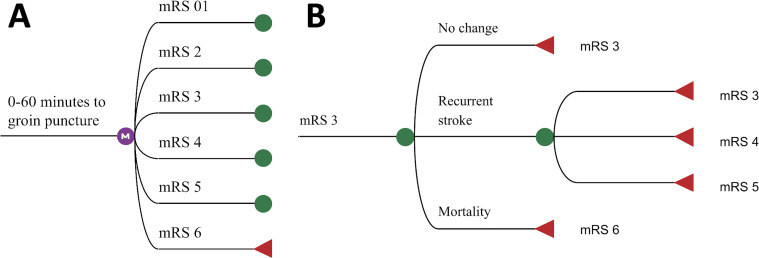
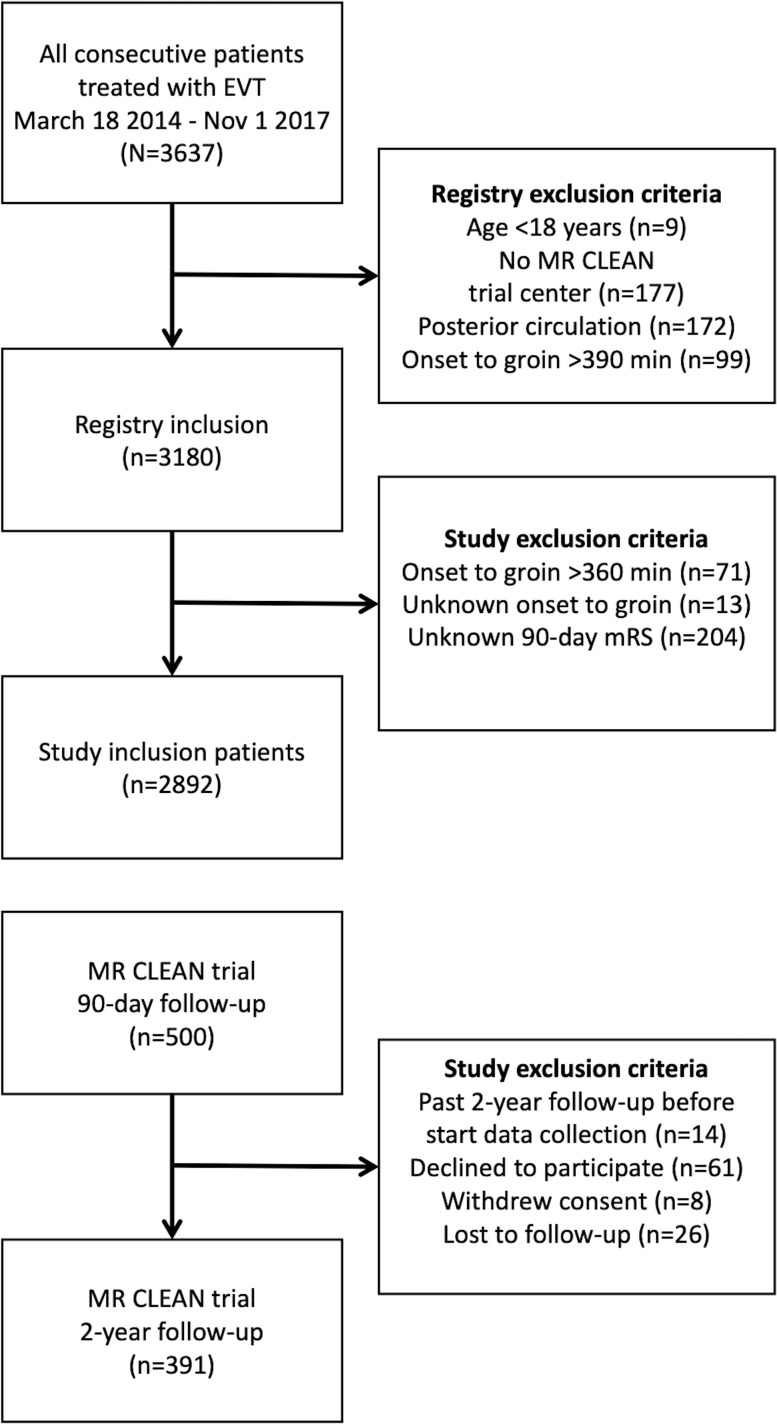
Methods: A Markov model was used to simulate 5-year follow-up functional outcome, measured with the modified Rankin Scale (mRS), of 69-year-old LVO patients. Post-treatment mRS was extracted from the MR CLEAN Registry (n=2892): costs per unit of time and Quality-Adjusted Life Years (QALYs) per mRS sub-score were retrieved from follow-up data of the MR CLEAN trial (n=500). Net Monetary Benefit (NMB) at a willingness to pay of €80 000 per QALY was reported as primary outcome, and secondary outcome measures were days of disability-free life gained and costs.
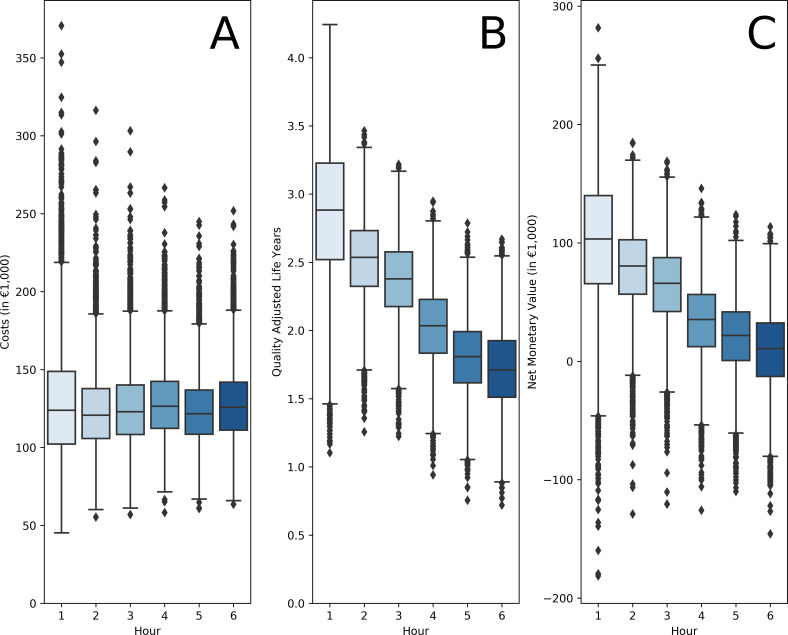
Results: EVT administered 1 min faster resulted in a median NMB of €309 (IQR: 226;389), 1.3 days of additional disability-free life (IQR: 1.0;1.6), while cumulative costs remained largely unchanged (median: -€15, IQR: -65;33) over a 5-year follow-up period. As costs over the follow-up period remained stable while QALYs decreased with longer time to treatment, which this results in a near-linear decrease of NMB. Since patients with faster EVT lived longer, they incurred more healthcare costs.
Conclusion: One-minute faster EVT increases QALYs while cumulative costs remain largely unaffected. Therefore, faster EVT provides better value of care at no extra healthcare costs.
Keywords: artery; economics; intervention; stroke; thrombectomy.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: DD and AvdL received funding from the Dutch Heart Foundation, Brain Foundation Netherlands, The Netherlands Organization for Health Research and Development, Health Holland Top Sector Life Sciences & Health, and unrestricted grants from Penumbra Inc., Stryker, Medtronic, Thrombolytic Science, and Cerenovus for research, all paid to institution. Consultation fees were received by DD and AvdL from Stryker and Bracco Imaging. Amsterdam UMC received a grant from Stryker for research led by CM and YR. CM, YR, and HM are shareholders of Nico.lab. Maastricht University MC received funds from Stryker and Cerenovus for consultations by WvZ. MG received consultation fees from Medtronic, Stryker, Microvention, and Mentice. Radboud UMC received funds from Stryker for consultations by Hieronymus Boogaarts.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials