

Two-dimensional shear wave elastography predicts survival in advanced chronic liver disease
- PMID: 33479052
- PMCID: PMC8761995
- DOI: 10.1136/gutjnl-2020-323419
Two-dimensional shear wave elastography predicts survival in advanced chronic liver disease
Abstract
Objective: Liver stiffness measurement (LSM) is a tool used to screen for significant fibrosis and portal hypertension. The aim of this retrospective multicentre study was to develop an easy tool using LSM for clinical outcomes in advanced chronic liver disease (ACLD) patients.
Design: This international multicentre cohort study included a derivation ACLD patient cohort with valid two-dimensional shear wave elastography (2D-SWE) results. Clinical and laboratory parameters at baseline and during follow-up were recorded. LSM by transient elastography (TE) was also recorded if available. The primary outcome was overall mortality. The secondary outcome was the development of first/further decompensation.
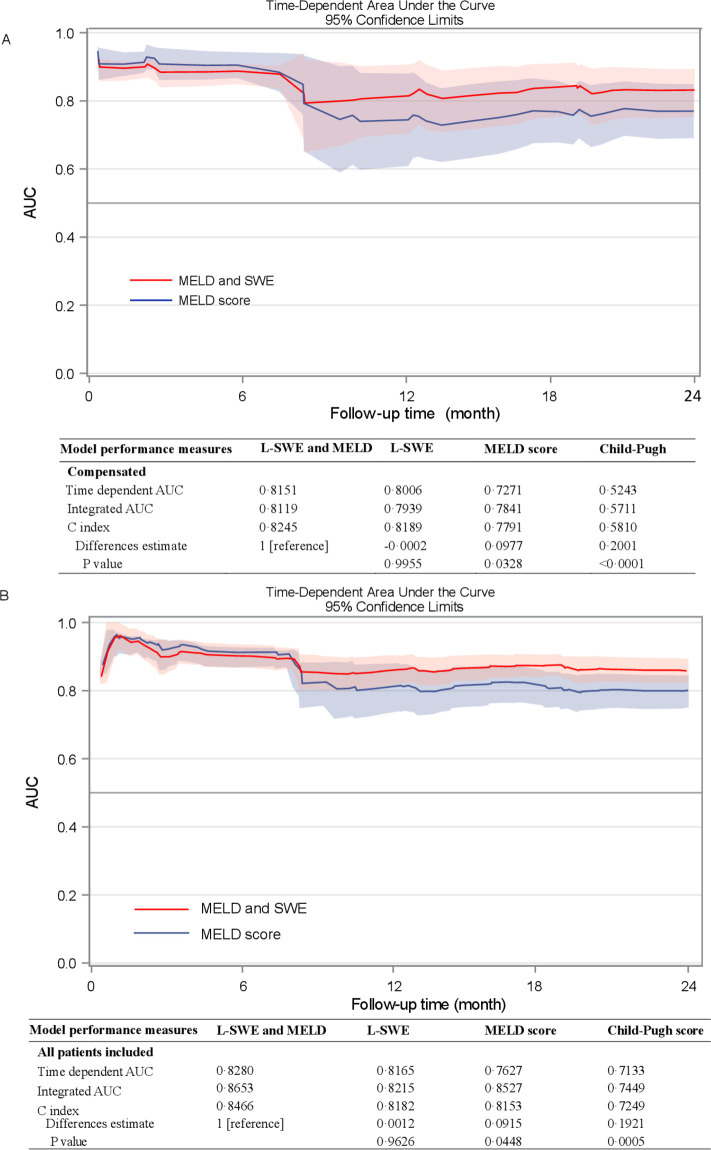
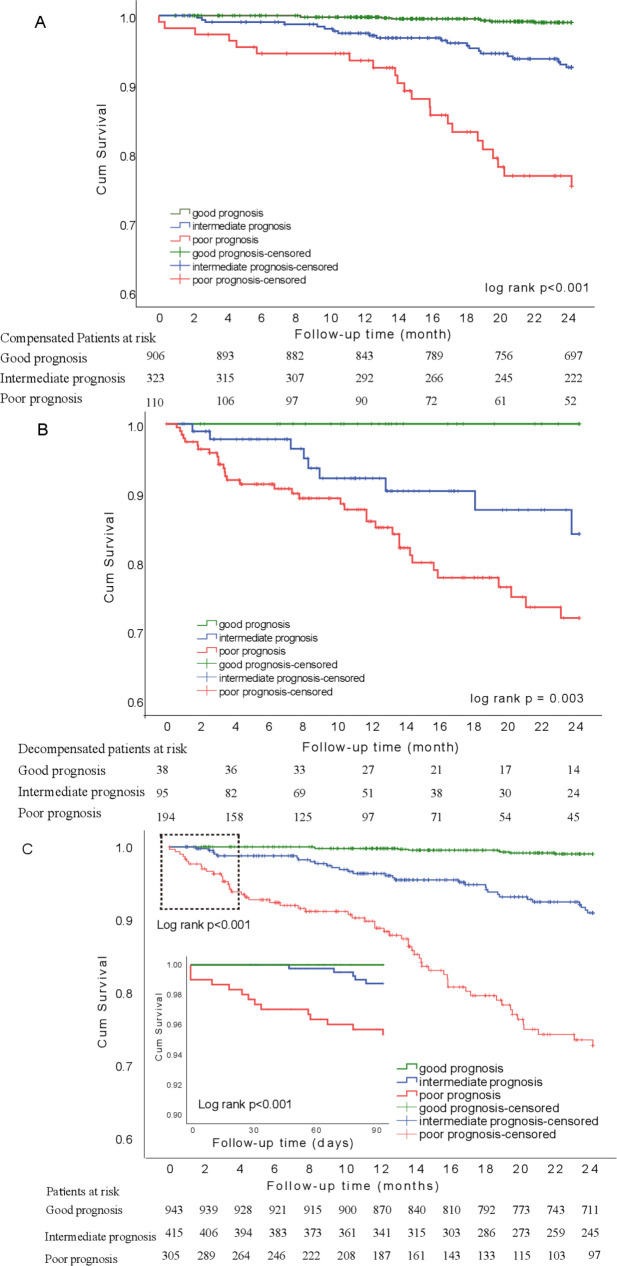
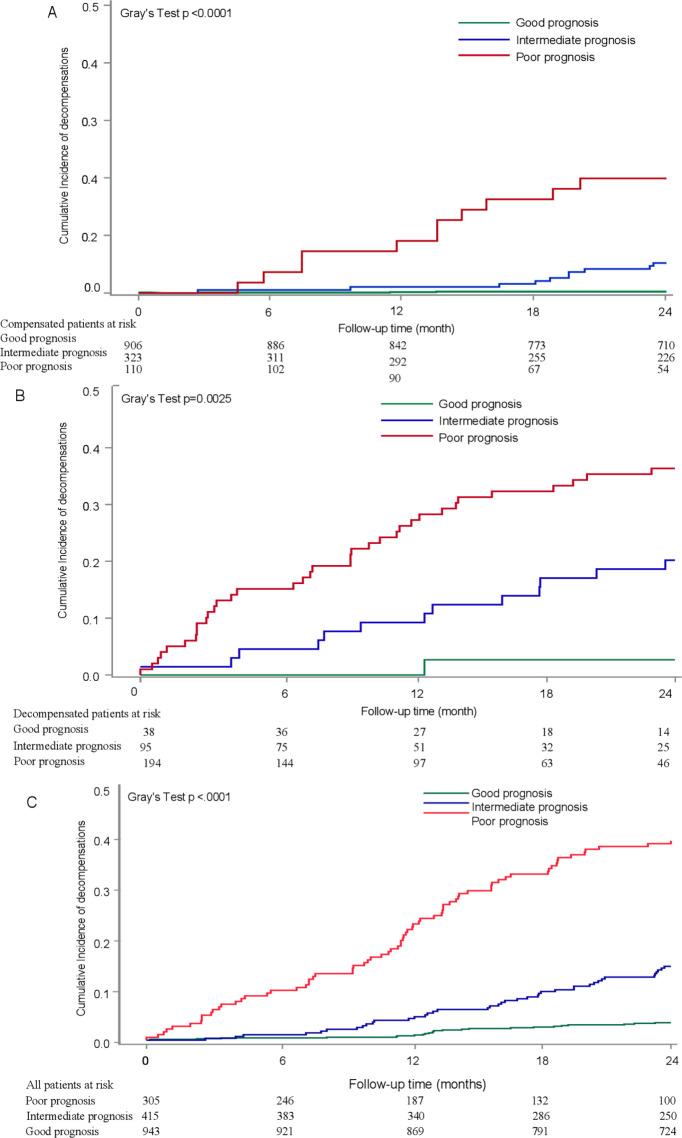
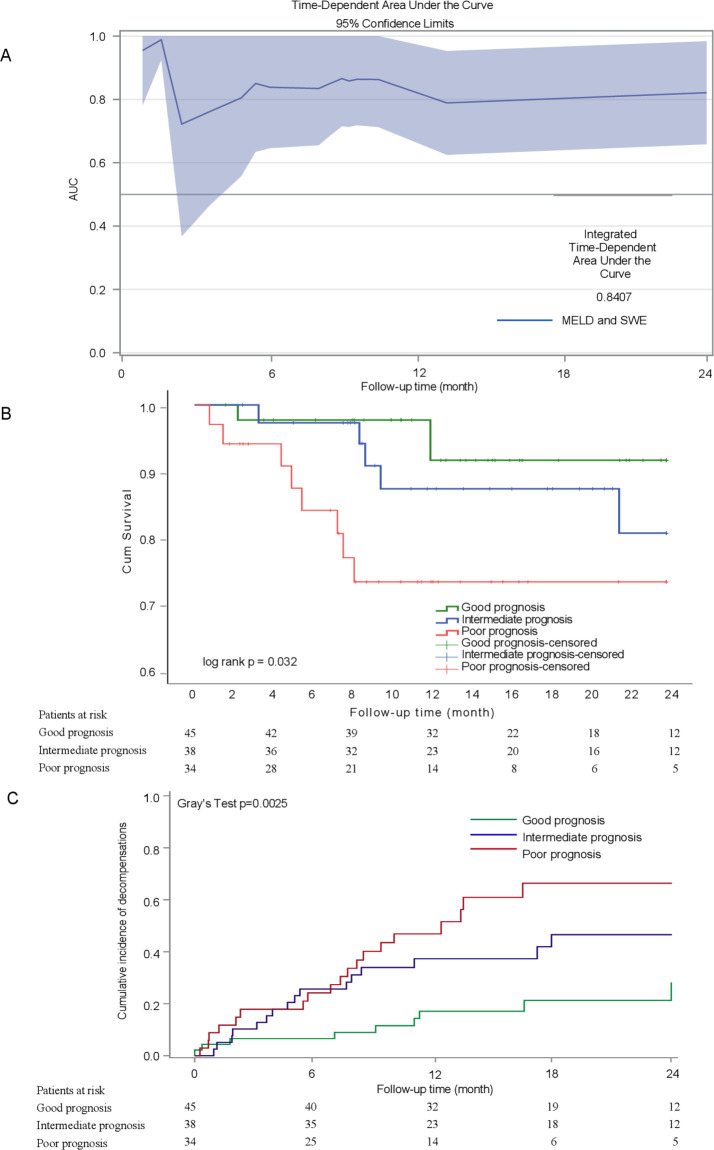
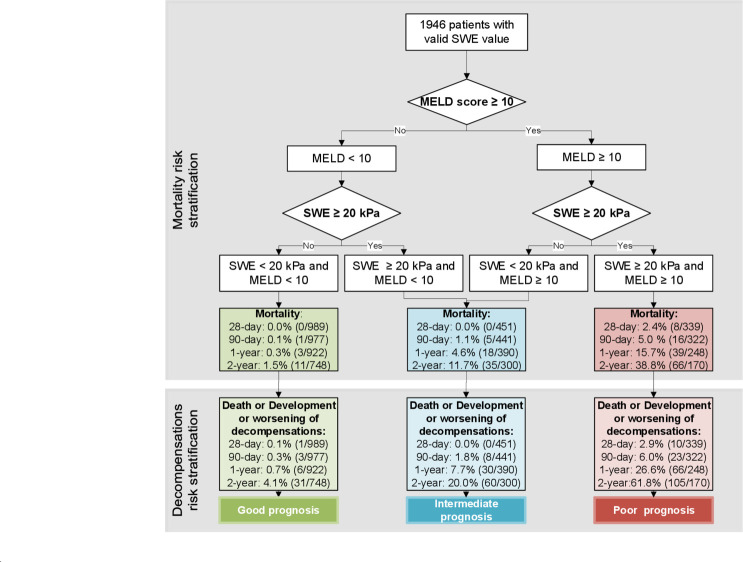
Results: After screening 2148 patients (16 centres), 1827 patients (55 years, 62.4% men) were included in the 2D-SWE cohort, with median liver SWE (L-SWE) 11.8 kPa and a model for end stage liver disease (MELD) score of 8. Combination of MELD score and L-SWE predict independently of mortality (AUC 0.8). L-SWE cut-off at ≥20 kPa combined with MELD ≥10 could stratify the risk of mortality and first/further decompensation in ACLD patients. The 2-year mortality and decompensation rates were 36.9% and 61.8%, respectively, in the 305 (18.3%) high-risk patients (with L-SWE ≥20 kPa and MELD ≥10), while in the 944 (56.6%) low-risk patients, these were 1.1% and 3.5%, respectively. Importantly, this M10LS20 algorithm was validated by TE-based LSM and in an additional cohort of 119 patients with valid point shear SWE-LSM.
Conclusion: The M10LS20 algorithm allows risk stratification of patients with ACLD. Patients with L-SWE ≥20 kPa and MELD ≥10 should be followed closely and receive intensified care, while patients with low risk may be managed at longer intervals.
Keywords: chronic liver disease; clinical decision making; liver cirrhosis; liver failure; portal hypertension.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JT has received speaking and/or consulting fees from Gore, Bayer, Alexion, MSD, Gilead, Intercept, Norgine, Grifols, Versantis, and Martin Pharmaceutical. Philip Ferstl received consultancy for SNIPR Biome. Supersonic Imagine supported interaction within the groups, but without specific funding.
Figures
Comment in
-
Beyond the AJR: "Two-Dimensional Shear Wave Elastography Predicts Survival in Advanced Chronic Liver Disease".AJR Am J Roentgenol. 2021 Oct;217(4):1012. doi: 10.2214/AJR.21.25821. Epub 2021 Mar 17. AJR Am J Roentgenol. 2021. PMID: 33728973 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical